

ACTIVExtend: 24 Months of Alendronate After 18 Months of Abaloparatide or Placebo for Postmenopausal Osteoporosis
- PMID: 29800372
- PMCID: PMC6097601
- DOI: 10.1210/jc.2018-00163
ACTIVExtend: 24 Months of Alendronate After 18 Months of Abaloparatide or Placebo for Postmenopausal Osteoporosis
Abstract
Purpose: In women with postmenopausal osteoporosis, we investigated the effects of 24 months of treatment with alendronate (ALN) following 18 months of treatment with abaloparatide (ABL) or placebo (PBO).
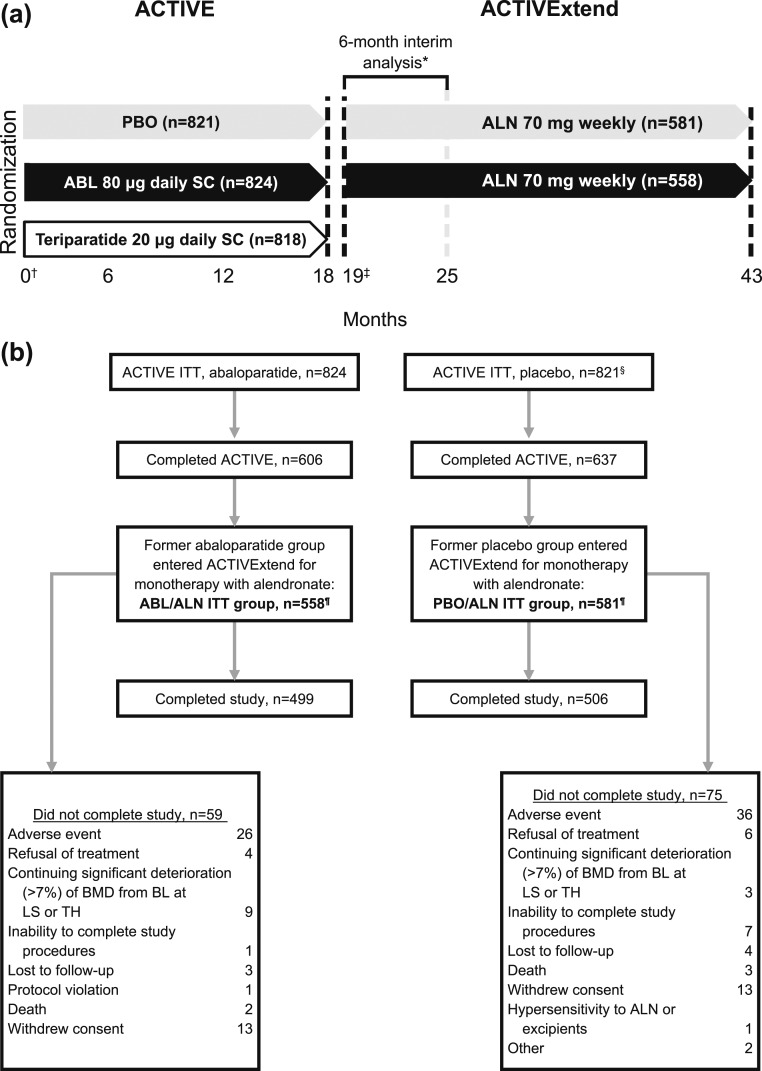
Methods: Women who completed ABL or PBO treatment in ACTIVE were eligible to receive up to 24 months of ALN. We evaluated the incidence of vertebral and nonvertebral fractures and changes in bone mineral density (BMD) during the entire 43-month period from ACTIVE baseline to the end of ACTIVExtend and for the 24-month extension only.
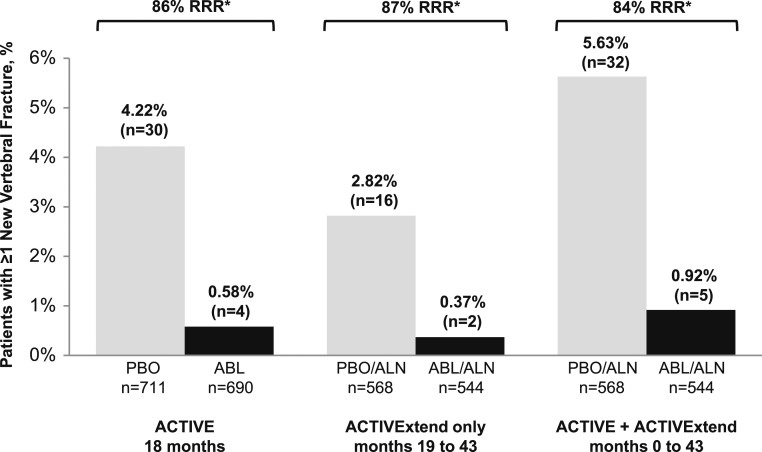
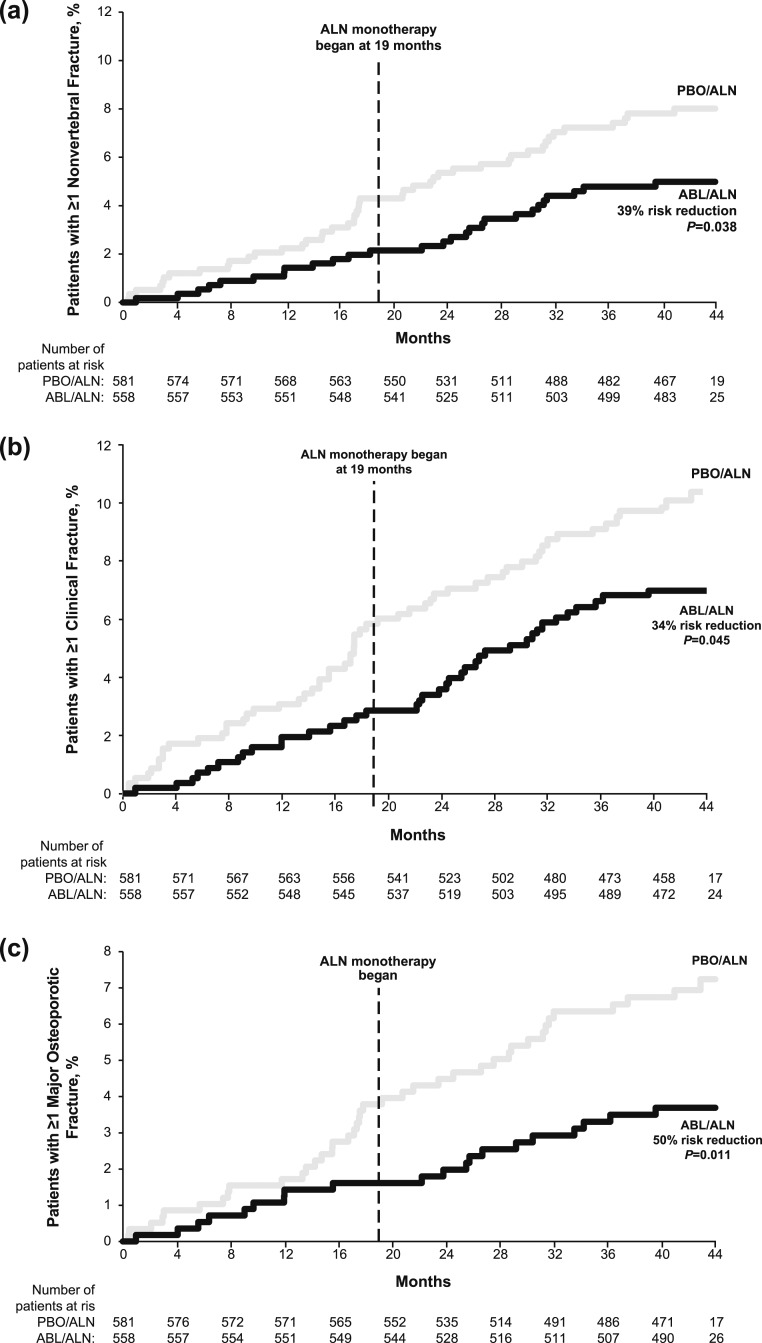
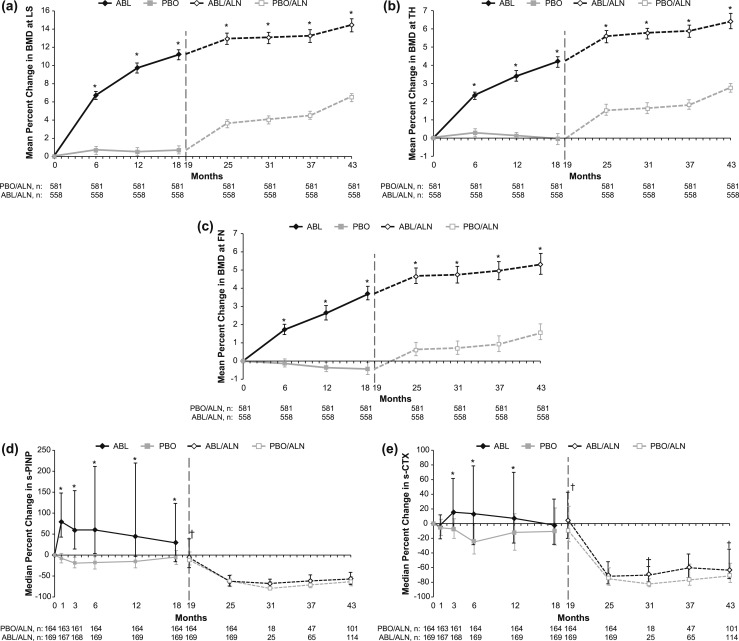
Results: Five hundred fifty-eight women from ACTIVE's ABL group and 581 from its PBO group (92% of ABL and PBO completers) were enrolled. During the full 43-month treatment period, 0.9% of evaluable women in the ABL/ALN group experienced a new radiographic vertebral fracture vs 5.6% of women in the PBO/ALN group, an 84% relative risk reduction (RRR, P < 0.001). Kaplan-Meier incidence rates for other reported fracture types were significantly lower for ABL/ALN vs PBO/ALN (all P < 0.05). Gains in BMD achieved during ACTIVE were further increased during ACTIVExtend. For ACTIVExtend only, RRR for vertebral fractures was 87% with ABL/ALN vs PBO/ALN (P = 0.001). Adverse events were similar between groups. A supplemental analysis for regulatory authorities found no hip fractures in the ABL/ALN group vs five in the PBO/ALN group.
Conclusions: Eighteen months of ABL followed by 24 months of ALN reduced the risk of vertebral, nonvertebral, clinical, and major osteoporotic fractures and increased BMD. Sequential ABL followed by ALN appears to be an effective treatment option for postmenopausal women at risk for osteoporosis-related fractures.
Trial registration: ClinicalTrials.gov NCT01657162.
Figures
References
-
- Seeman E, Martin TJ. Co-administration of antiresorptive and anabolic agents: a missed opportunity. J Bone Miner Res. 2015;30(5):753–764. - PubMed
-
- Leder BZ, Tsai JN, Jiang LA, Lee H. Importance of prompt antiresorptive therapy in postmenopausal women discontinuing teriparatide or denosumab: The Denosumab and Teriparatide Follow-up Study (DATA-Follow-up). Bone. 2017;98:54–58. - PubMed
-
- Rittmaster RS, Bolognese M, Ettinger MP, Hanley DA, Hodsman AB, Kendler DL, Rosen CJ. Enhancement of bone mass in osteoporotic women with parathyroid hormone followed by alendronate. J Clin Endocrinol Metab. 2000;85(6):2129–2134. - PubMed
-
- Black DM, Greenspan SL, Ensrud KE, Palermo L, McGowan JA, Lang TF, Garnero P, Bouxsein ML, Bilezikian JP, Rosen CJ; PaTH Study Investigators . The effects of parathyroid hormone and alendronate alone or in combination in postmenopausal osteoporosis. N Engl J Med. 2003;349(13):1207–1215. - PubMed
-
- Black DM, Bilezikian JP, Ensrud KE, Greenspan SL, Palermo L, Hue T, Lang TF, McGowan JA, Rosen CJ; PaTH Study Investigators . One year of alendronate after one year of parathyroid hormone (1–84) for osteoporosis. N Engl J Med. 2005;353(6):555–565. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
