

Computer-Based Driving in Dementia Decision Tool With Mail Support: Cluster Randomized Controlled Trial
- PMID: 29802093
- PMCID: PMC5993977
- DOI: 10.2196/jmir.9126
Computer-Based Driving in Dementia Decision Tool With Mail Support: Cluster Randomized Controlled Trial
Abstract
Background: Physicians often find significant challenges in assessing automobile driving in persons with mild cognitive impairment and mild dementia and deciding when to report to transportation administrators. Care must be taken to balance the safety of patients and other road users with potential negative effects of issuing such reports.
Objective: The aim of this study was to assess whether a computer-based Driving in Dementia Decision Tool (DD-DT) increased appropriate reporting of patients with mild dementia or mild cognitive impairment to transportation administrators.
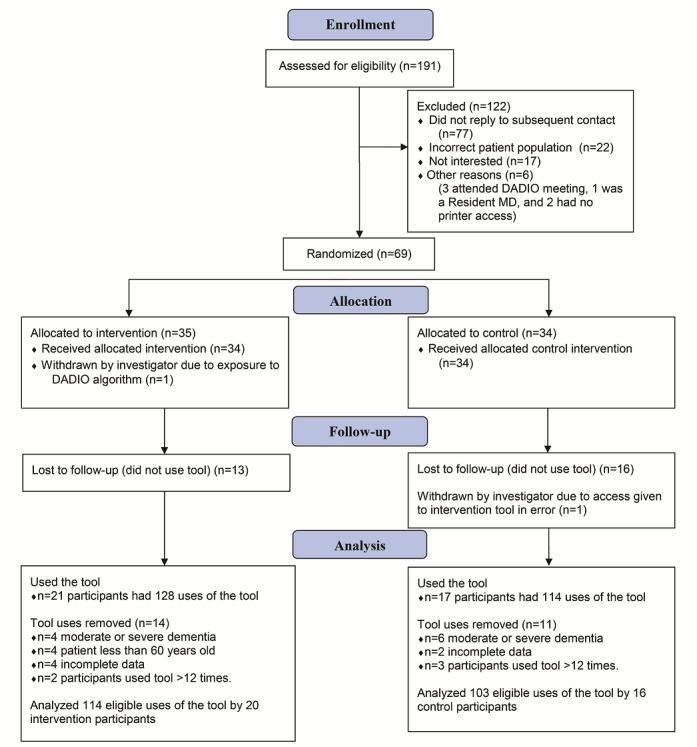
Methods: The study used a parallel-group cluster nonblinded randomized controlled trial design to test a multifaceted knowledge translation intervention. The intervention included a computer-based decision support system activated by the physician-user, which provides a recommendation about whether to report patients with mild dementia or mild cognitive impairment to transportation administrators, based on an algorithm derived from earlier work. The intervention also included a mailed educational package and Web-based specialized reporting forms. Specialists and family physicians with expertise in dementia or care of the elderly were stratified by sex and randomized to either use the DD-DT or a control version of the tool that required identical data input as the intervention group, but instead generated a generic reminder about the reporting legislation in Ontario, Canada. The trial ran from September 9, 2014 to January 29, 2016, and the primary outcome was the number of reports made to the transportation administrators concordant with the algorithm.
Results: A total of 69 participating physicians were randomized, and 36 of these used the DD-DT; 20 of the 35 randomized to the intervention group used DD-DT with 114 patients, and 16 of the 34 randomized to the control group used it with 103 patients. The proportion of all assessed patients reported to the transportation administrators concordant with recommendation did not differ between the intervention and the control groups (50% vs 49%; Z=-0.19, P=.85). Two variables predicted algorithm-based reporting-caregiver concern (odds ratio [OR]=5.8, 95% CI 2.5-13.6, P<.001) and abnormal clock drawing (OR 6.1, 95% CI 3.1-11.8, P<.001).
Conclusions: On the basis of this quantitative analysis, in-office abnormal clock drawing and expressions of concern about driving from caregivers substantially influenced physicians to report patients with mild dementia or mild cognitive impairment to transportation administrators, but the DD-DT tool itself did not increase such reports among these expert physicians.
Trial registration: ClinicalTrials.gov NCT02036099; https://clinicaltrials.gov/ct2/show/NCT02036099 (Archived by WebCite at http://www.webcitation.org/6zGMF1ky8).
Keywords: automobile driving; decision support systems, clinical; dementia; mild cognitive impairment.
©Mark J Rapoport, Carla Zucchero Sarracini, Alex Kiss, Linda Lee, Anna Byszewski, Dallas P Seitz, Brenda Vrkljan, Frank Molnar, Nathan Herrmann, David F Tang-Wai, Christopher Frank, Blair Henry, Nicholas Pimlott, Mario Masellis, Gary Naglie. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 25.05.2018.
Conflict of interest statement
Conflicts of Interest: DPS has participated in clinical trials sponsored by Roche Pharmaceuticals.
Figures
References
-
- World Health Organization. Geneva: World Health Organization; 2013. [2017-06-23]. Global status report on road safety 2013: supporting a decade of action http://www.who.int/violence_injury_prevention/road_safety_status/2013/en/
-
- Peden M, Scurfield R, Sleet D, Mohan D, Hyder A, et al. World Health Organization. Geneva: World Health Organization; 2004. [2017-06-23]. World report on road traffic injury prevention http://www.who.int/violence_injury_prevention/publications/road_traffic/...
-
- Li G, Braver ER, Chen LH. Fragility versus excessive crash involvement as determinants of high death rates per vehicle-mile of travel among older drivers. Accid Anal Prev. 2003 Mar;35(2):227–35.S0001457501001075 - PubMed
-
- Langford J, Charlton JL, Koppel S, Myers A, Tuokko H, Marshall S, Man-Son-Hing M, Darzins P, Di SM, Macdonald W. Findings from the Candrive/Ozcandrive study: low mileage older drivers, crash risk and reduced fitness to drive. Accid Anal Prev. 2013 Dec;61:304–10. doi: 10.1016/j.aap.2013.02.006.S0001-4575(13)00035-3 - DOI - PubMed
-
- Dobbs BM, Carr DB, Morris JC. Evaluation and management of the driver with dementia. Neurologist. 2002 Mar;8(2):61–70. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
