

Model for Prediction of Optimal Debulking of Epithelial Ovarian Cancer
- PMID: 29802693
- PMCID: PMC6031811
- DOI: 10.22034/APJCP.2018.19.5.1319
Model for Prediction of Optimal Debulking of Epithelial Ovarian Cancer
Abstract
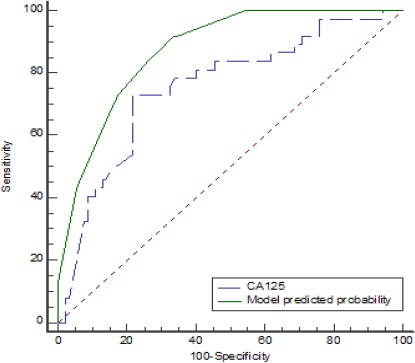
Background: Primary cytoreduction surgery followed by chemotherapy is the cornerstone treatment for epithelial ovarian cancer (EOC). In patients with a low probability of optimal primary surgical debulking, neoadjuvant chemotherapy (NACT) followed by interval debulking increases the chance of optimal surgery. The aim of this study was to develop a model to identify preoperative predictors for suboptimal cytoreduction. Methods: Medical records of patients with EOC who underwent primary cytoreductive surgery in a referral tertiary gyneco-oncology center were reviewed from 2007 to 2017. Data were collected on a range of characteristics including demographic features, comorbidities, serum tumor markers, hematologic markers, preoperative imaging, surgical procedures, and pathologic reports. Univariate and multivariate analyses were performed to clarify the ability of preoperative factors to predict suboptimal primary surgery. Results: The majority of patients (71.3%) who underwent primary cytoreductive surgery were optimally debulked. Based on the Youden index, the best cut-off point for the serum CA125 level to distinguish suboptimal debulking was 420U/ml with 0.730 (95%CI:0.559 to 0.862) sensitivity and 0.783 (0.684 to 0.862) specificity. Multiple logistic regression results showed that serum CA125 level >420 U/ ml (p value <0.001), the presence of liver metastasis on preoperative imaging (p value: 0.041) and ascites (p value: 0.032) or massive ascites (p value:0.010) significantly increased the risk of suboptimal debulking (logit p = 2.36 CA125 level +1.85 Liverinvolvement +1.68 presence of Ascites+ 2.28 Massive Ascites). Conclusion:The present study suggests that a serum CA125 level >420 U/ml, the presence of ascites or massive ascites and liver metastasis are strong predictors of suboptimal primary surgery in cases of EOC. Based on the constructed model, with any of these 4 factors, the probability of suboptimal debulking in EOC is more than 80%.
Keywords: Optimal debulking; neoadjuant chemotherapy; CA125; prediction model.
Creative Commons Attribution License
Figures
Similar articles
-
Serum HE4 superior to CA125 in predicting poorer surgical outcome of epithelial ovarian cancer.Tumour Biol. 2016 Nov;37(11):14765-14772. doi: 10.1007/s13277-016-5335-0. Epub 2016 Sep 15. Tumour Biol. 2016. PMID: 27629144
-
Preoperative serum CA125 levels do not predict suboptimal cytoreductive surgery in epithelial ovarian cancer.Int J Gynecol Cancer. 2008 Jul-Aug;18(4):621-8. doi: 10.1111/j.1525-1438.2007.01064.x. Epub 2007 Sep 14. Int J Gynecol Cancer. 2008. PMID: 17868339
-
Serum CA125 levels predict outcome of interval debulking surgery after neoadjuvant chemotherapy in patients with advanced ovarian cancer.Clin Chim Acta. 2018 Sep;484:32-35. doi: 10.1016/j.cca.2018.04.030. Epub 2018 Apr 24. Clin Chim Acta. 2018. PMID: 29702068
-
[Diagnostic and prognostic value of tumor markers, scores (clinical and biological) algorithms, in front of an ovarian mass suspected of an epithelial ovarian cancer: Article drafted from the French Guidelines in oncology entitled "Initial management of patients with epithelial ovarian cancer" developed by FRANCOGYN, CNGOF, SFOG, GINECO-ARCAGY under the aegis of CNGOF and endorsed by INCa].Gynecol Obstet Fertil Senol. 2019 Feb;47(2):134-154. doi: 10.1016/j.gofs.2018.12.013. Epub 2019 Feb 5. Gynecol Obstet Fertil Senol. 2019. PMID: 30733191 Review. French.
-
Primary debulking surgery and neoadjuvant chemotherapy in the treatment of advanced epithelial ovarian carcinoma.Cancer Metastasis Rev. 2015 Mar;34(1):5-10. doi: 10.1007/s10555-014-9536-y. Cancer Metastasis Rev. 2015. PMID: 25597035 Review.
Cited by
-
Surgery in Advanced Ovary Cancer: Primary versus Interval Cytoreduction.Diagnostics (Basel). 2022 Apr 14;12(4):988. doi: 10.3390/diagnostics12040988. Diagnostics (Basel). 2022. PMID: 35454036 Free PMC article. Review.
-
Lifestyle and personal factors associated with having macroscopic residual disease after ovarian cancer primary cytoreductive surgery.Gynecol Oncol. 2023 Jan;168:68-75. doi: 10.1016/j.ygyno.2022.10.018. Epub 2022 Nov 17. Gynecol Oncol. 2023. PMID: 36401943 Free PMC article.
-
The Use of Artificial Intelligence for Complete Cytoreduction Prediction in Epithelial Ovarian Cancer: A Narrative Review.Cancer Control. 2023 Jan-Dec;30:10732748231159553. doi: 10.1177/10732748231159553. Cancer Control. 2023. PMID: 36847148 Free PMC article. Review.
-
The Role of Interleukin 6 (IL6), Cancer Antigen-125 (CA-125), and Human Epididymis Protein 4 (HE4) to predict tumor resectability in the advanced epithelial ovarian cancer patients.PLoS One. 2023 Oct 4;18(10):e0292282. doi: 10.1371/journal.pone.0292282. eCollection 2023. PLoS One. 2023. PMID: 37792745 Free PMC article.
-
Preoperative Predictors of Optimal Tumor Resectability in Patients With Epithelial Ovarian Cancer.Cureus. 2022 Jan 19;14(1):e21409. doi: 10.7759/cureus.21409. eCollection 2022 Jan. Cureus. 2022. PMID: 35198316 Free PMC article.
References
-
- Arab M, Noghabaei G. Ovarian cancer incidence in Iran and the world. Rep Pract Oncol Radiother. 2013;1:67–72.
-
- Ashrafganjoei T, Mohamadianamiri M, Farzaneh F, et al. Investigating preoperative hematologic markers for prediction of ovarian cancer surgical outcome. Asian Pac J Cancer Prev. 2016;17:1445–8. - PubMed
-
- Axtell AE, Lee MH, Bristow RE, et al. Multi-institutional reciprocal validation study of computed tomography predictors of suboptimal primary cytoreduction in patients with advanced ovarian cancer. J Clin Oncol. 2007;25:384–9. - PubMed
-
- Bristow RE, Tomacruz RS, Armstrong DK, et al. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era:a meta-analysis. J Clin Oncol. 2002;20:1248–59. - PubMed
-
- Brockbank E, Ind T, Barton D, et al. Preoperative predictors of suboptimal primary surgical cytoreduction in women with clinical evidence of advanced primary epithelial ovarian cancer. Int J Gynecol Cancer. 2004;14:42–50. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous