

Effect of a Patient and Clinician Communication-Priming Intervention on Patient-Reported Goals-of-Care Discussions Between Patients With Serious Illness and Clinicians: A Randomized Clinical Trial
- PMID: 29802770
- PMCID: PMC6145723
- DOI: 10.1001/jamainternmed.2018.2317
Effect of a Patient and Clinician Communication-Priming Intervention on Patient-Reported Goals-of-Care Discussions Between Patients With Serious Illness and Clinicians: A Randomized Clinical Trial
Abstract
Importance: Clinician communication about goals of care is associated with improved patient outcomes and reduced intensity of end-of-life care, but it is unclear whether interventions can improve this communication.
Objective: To evaluate the efficacy of a patient-specific preconversation communication-priming intervention (Jumpstart-Tips) targeting both patients and clinicians and designed to increase goals-of-care conversations compared with usual care.
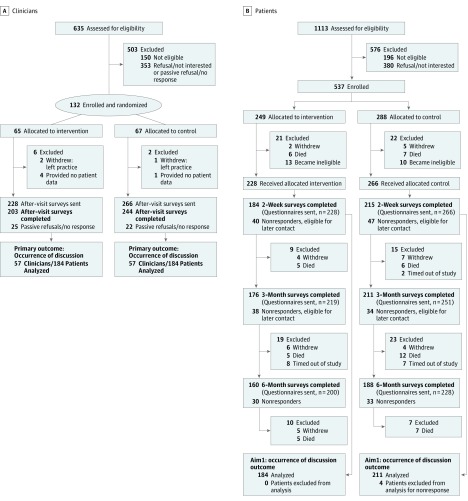
Design, setting, and participants: Multicenter cluster-randomized trial in outpatient clinics with physicians or nurse practitioners and patients with serious illness. The study was conducted between 2012 and 2016.
Interventions: Clinicians were randomized to the bilateral, preconversation, communication-priming intervention (n = 65) or usual care (n = 67), with 249 patients assigned to the intervention and 288 to usual care.
Main outcomes and measures: The primary outcome was patient-reported occurrence of a goals-of-care conversation during a target outpatient visit. Secondary outcomes included clinician documentation of a goals-of-care conversation in the medical record and patient-reported quality of communication (Quality of Communication questionnaire [QOC]; 4-indicator latent construct) at 2 weeks, as well as patient assessments of goal-concordant care at 3 months and patient-reported symptoms of depression (8-item Patient Health Questionnaire; PHQ-8) and anxiety (7-item Generalized Anxiety Disorder survey; GAD-7) at 3 and 6 months. Analyses were clustered by clinician and adjusted for confounders.
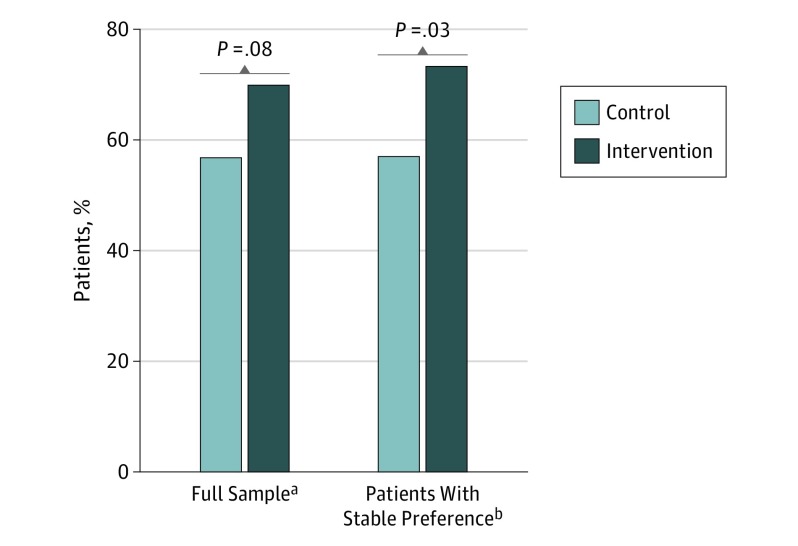
Results: We enrolled 132 of 485 potentially eligible clinicians (27% participation; 71 women [53.8%]; mean [SD] age, 47.1 [9.6] years) and 537 of 917 eligible patients (59% participation; 256 women [47.7%]; mean [SD] age, 73.4 [12.7] years). The intervention was associated with a significant increase in a goals-of-care discussion at the target visit (74% vs 31%; P < .001) and increased medical record documentation (62% vs 17%; P < .001), as well as increased patient-rated quality of communication (4.6 vs 2.1; P = .01). Patient-assessed goal-concordant care did not increase significantly overall (70% vs 57%; P = .08) but did increase for patients with stable goals between 3-month follow-up and last prior assessment (73% vs 57%; P = .03). Symptoms of depression or anxiety were not different between groups at 3 or 6 months.
Conclusions and relevance: This intervention increased the occurrence, documentation, and quality of goals-of-care communication during routine outpatient visits and increased goal-concordant care at 3 months among patients with stable goals, with no change in symptoms of anxiety or depression. Understanding the effect on subsequent health care delivery will require additional study.
Trial registration: ClinicalTrials.gov identifier: NCT01933789.
Conflict of interest statement
Figures
Comment in
-
Precision Communication-A Path Forward to Improve Goals-of-Care Communication.JAMA Intern Med. 2018 Jul 1;178(7):940-942. doi: 10.1001/jamainternmed.2018.2307. JAMA Intern Med. 2018. PMID: 29802771 No abstract available.
References
-
- Curtis JR, Engelberg RA, Nielsen EL, Au DH, Patrick DL. Patient-physician communication about end-of-life care for patients with severe COPD. Eur Respir J. 2004;24(2):200-205. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
