

Seronegative enteropathy and malnutrition: a diagnostic challenge
- PMID: 29804077
- PMCID: PMC5976131
- DOI: 10.1136/bcr-2018-224397
Seronegative enteropathy and malnutrition: a diagnostic challenge
Abstract
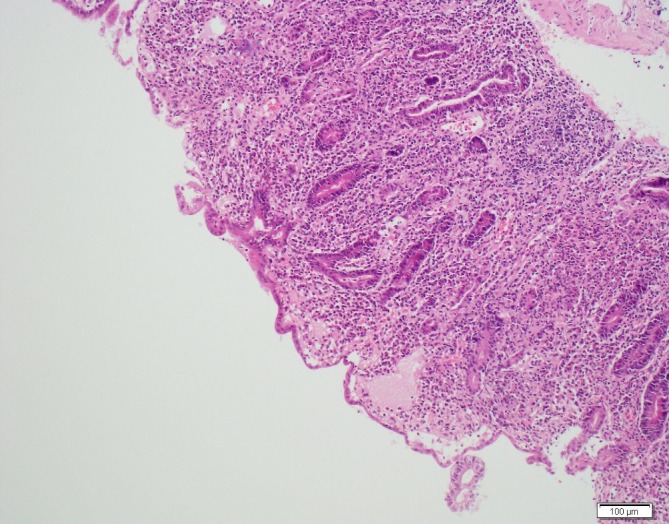
A 21-year-old woman presented with a 2-week history of vomiting, diarrhoea and epigastric pain, with 9 kg weight loss over the last two months. Laboratory tests were normal with negative coeliac serology. Duodenal biopsies revealed total villous atrophy, crypt hypertrophy and intraepithelial lymphocytosis. A diagnosis of seronegative coeliac disease was made, and she started a gluten-free diet. However, she did not respond and her weight fell to 30.6 kg (body mass index 11), becoming dependent on parenteral nutrition. Her diagnosis was reconsidered and the histology reviewed. The histopathological features were of severe active chronic duodenitis. By diagnosis of exclusion, with the absence of other clear pathology, she was treated as Crohn's disease. She responded to third-line therapy with biologics. In this case, the patient had refractory villous atrophy and the mucosal features, in addition to response with anti-tumour necrosis factor therapy, suggest inflammatory bowel disease, although not with complete diagnostic certainty.
Keywords: crohn’s disease; gastrointestinal system; malabsorption; malnutrition; parenteral / enteral feeding.
© BMJ Publishing Group Ltd (unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical