

Troponin T monitoring to detect myocardial injury after noncardiac surgery: a cost-consequence analysis
- PMID: 29806816
- PMCID: PMC5973906
- DOI: 10.1503/cjs.010217
Troponin T monitoring to detect myocardial injury after noncardiac surgery: a cost-consequence analysis
Abstract
Background: Myocardial injury after noncardiac surgery (MINS) is a mostly asymptomatic condition that is strongly associated with 30-day mortality; however, it remains mostly undetected without systematic troponin T monitoring. We evaluated the cost and consequences of postoperative troponin T monitoring to detect MINS.
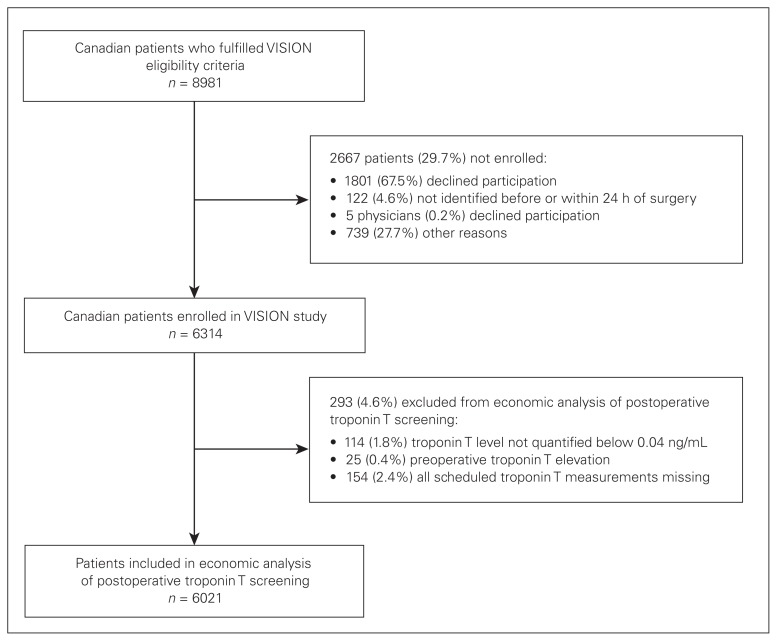
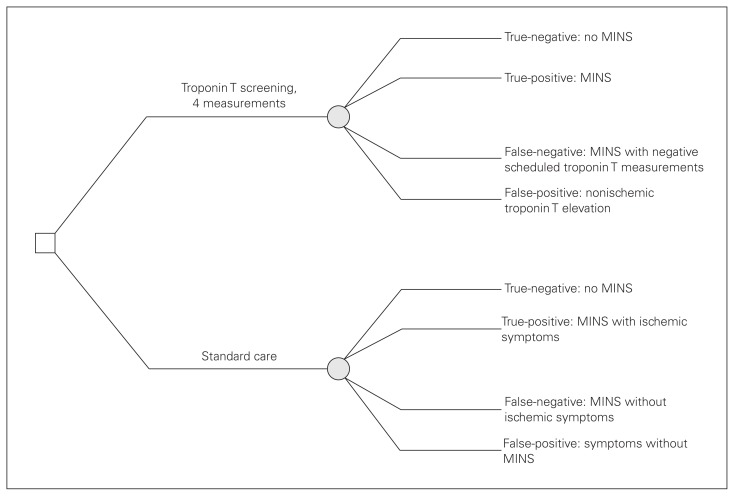
Methods: We conducted a model-based cost-consequence analysis to compare the impact of routine troponin T monitoring versus standard care (troponin T measurement triggered by ischemic symptoms) on the incidence of MINS detection. Model inputs were based on Canadian patients enrolled in the Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION) study, which enrolled patients aged 45 years or older undergoing inpatient noncardiac surgery. We conducted probability analyses with 10 000 iterations and extensive sensitivity analyses.
Results: The data were based on 6021 patients (48% men, mean age 65 [standard deviation 12] yr). The 30-day mortality rate for MINS was 9.6%. We determined the incremental cost to avoid missing a MINS event as $1632 (2015 Canadian dollars). The cost-effectiveness of troponin monitoring was higher in patient subgroups at higher risk for MINS, e.g., those aged 65 years or more, or with a history of atherosclerosis or diabetes ($1309).
Conclusion: The costs associated with a troponin T monitoring program to detect MINS were moderate. Based on the estimated incremental cost per health gain, implementation of postoperative troponin T monitoring seems appealing, particularly in patients at high risk for MINS.
Contexte: Les lésions myocardiques après chirurgie non cardiaque (CNC) sont majoritairement asymptomatiques et fortement associées au risque de mortalité dans les 30 jours; toutefois, dans la plupart des cas, elles ne sont pas détectées en l'absence d'une surveillance systématique de la troponine T. Nous avons évalué les coûts et les conséquences d'une telle surveillance pour détecter les lésions myocardiques après CNC.
Méthodes: Nous avons mené une analyse coût-conséquence modélisée pour comparer la surveillance systématique de la troponine T aux soins habituels seuls (mesure de la troponine T seulement s'il y a présence de symptômes d'ischémie) sur la fréquence de détection de lésions myocardiques après CNC. Les données ayant servi à l'analyse provenaient des patients canadiens ayant participé à l'étude de cohorte VISION, qui visait à évaluer les complications vasculaires chez les patients de 45 ans et plus ayant subi une CNC. Nous avons mené des analyses de probabilité avec 10 000 itérations et des analyses de sensibilité approfondies.
Résultats: Les données portaient sur 6021 patients (48 % du sexe masculin; âge moyen de 65 ans [écart-type de 12 ans]). Le taux de mortalité dans les 30 jours associé à une lésion myocardique après CNC était de 9,6 %. Nous avons déterminé que le coût marginal de la détection de la présence d'une lésion par surveillance de la troponine T était de 1632 $ (dollars canadiens en 2015). Le rapport coût-efficacité était plus bas pour les sous-groupes de patients à risque élevé de lésion myocardique après CNC, comme les patients de 65 ans et plus ou ceux ayant des antécédents d'athérosclérose ou de diabète (1309 $), que pour leurs pairs.
Conclusion: Les coûts associés à un programme de surveillance de la troponine T pour détecter les lésions myocardiques après CNC étaient modérés. Le coût marginal estimé par gain de santé indique que la mise en œuvre de ce type de programme pourrait être une option intéressante, surtout pour les patients à risque élevé de lésion myocardique après CNC.
Conflict of interest statement
Figures
References
-
- Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008;372:139–44. - PubMed
-
- Botto F, Alonso-Coello P, Chan MT, et al. Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Writing Group, on behalf of The Vascular events In noncardiac Surgery patIents cOhort evaluatioN (VISION) Investigators. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120:564–78. - PubMed
-
- Devereaux PJ, Xavier D, Pogue J, et al. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Intern Med. 2011;154:523–8. - PubMed
-
- Foucrier A, Rodseth R, Aissaoui M, et al. The long-term impact of early cardiovascular therapy intensification for postoperative troponin elevation after major vascular surgery. Anesth Analg. 2014;119:1053–63. - PubMed
-
- Duceppe E, Parlow J, MacDonald P, et al. Canadian Cardiovascular Society Guidelines on Perioperative Cardiac Risk Assessment and Management for Patients Who Undergo Noncardiac Surgery. Can J Cardiol. 2017;33:17–32. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical