

Risk-stratified clinical pathways decrease the duration of hospitalization and costs of perioperative care after pancreatectomy
- PMID: 29807648
- PMCID: PMC7265789
- DOI: 10.1016/j.surg.2018.04.014
Risk-stratified clinical pathways decrease the duration of hospitalization and costs of perioperative care after pancreatectomy
Abstract
Background: Postoperative pancreatic fistula is associated with adverse events, increased duration of stay and hospital costs. We developed perioperative care pathways stratified by postoperative pancreatic fistula risk with the aims of minimizing variations in care, improving quality, and decreasing costs.
Study design: Three unique risk-stratified pancreatectomy clinical pathways-low-risk pancreatoduodenectomy, high-risk pancreatoduodenectomy, and distal pancreatectomy were developed and implemented. Consecutive patients treated after implementation of the risk-stratified pancreatectomy clinical pathways were compared with patients treated immediately prior. Duration of stay, rates of perioperative adverse effects, discharge disposition, and hospital readmission, as well as the associated costs of care, were evaluated.
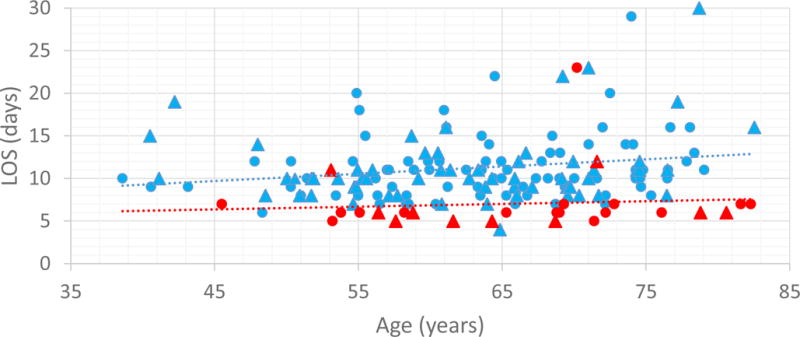
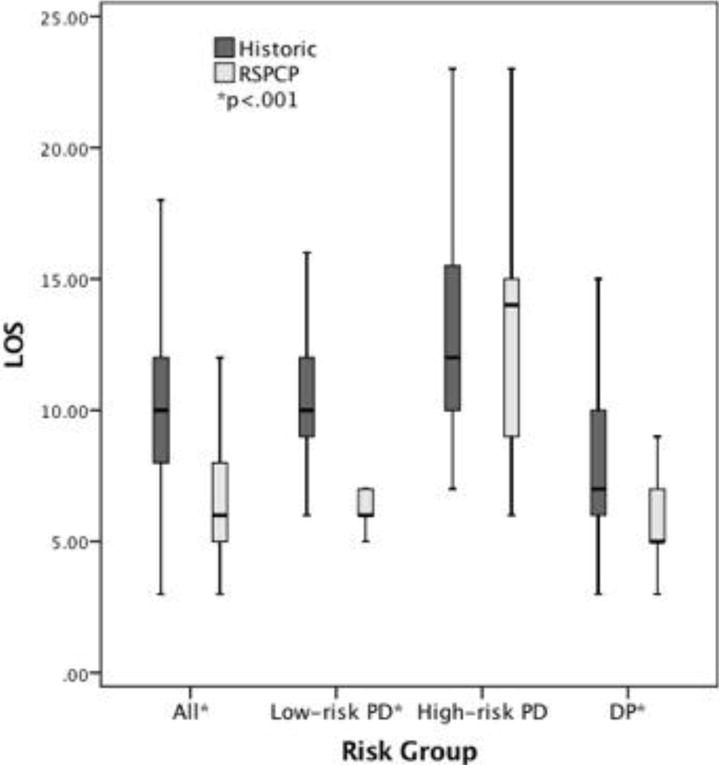
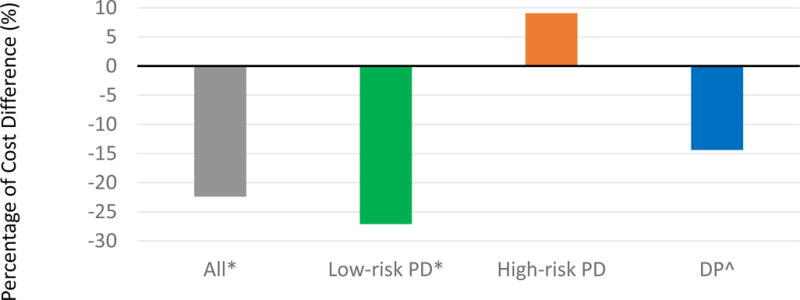
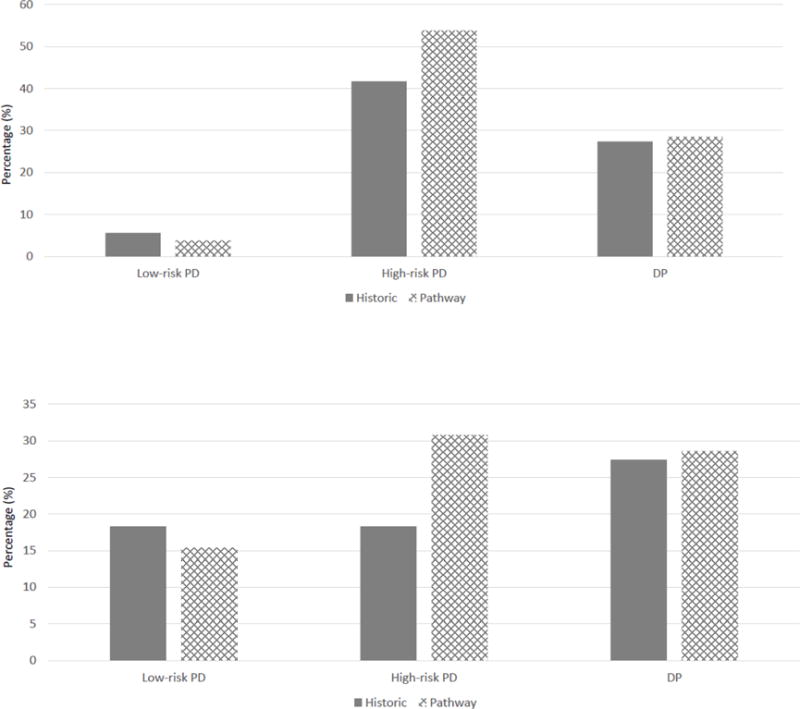
Results: The median hospital stay after pancreatectomy decreased from 10 to 6 days after implementation of the risk-stratified pancreatectomy clinical pathways (P < .001), and the median cost of index hospitalization decreased by 22%. Decreased changes in median hospital stay and costs of hospitalization were observed in association with low-risk pancreatoduodenectomy (P < .05) and distal pancreatectomy (P < .05), but not high-risk pancreatoduodenectomy. The rates of 90-day adverse events, grade B/C postoperative pancreatic fistula, discharge to a facility other than home, or readmission did not change after implementation.
Conclusion: Implementation of risk-stratified pancreatectomy clinical pathways decreased median stay and cost of index hospitalization after pancreatectomy without unfavorably affecting rates of perioperative adverse events or readmission, or discharge disposition. Outcomes were most favorably improved for low-risk pancreatoduodenectomy and distal pancreatectomy. Additional work is necessary to decrease the rate of postoperative pancreatic fistula, minimize variability, and improve outcomes after high-risk pancreatoduodenectomy.
Published by Elsevier Inc.
Conflict of interest statement
Conflict of interest: none
Figures
References
-
- Wood T, Aarts MA, Okrainec A, et al. Emergency Room Visits and Readmissions Following Implementation of an Enhanced Recovery After Surgery (iERAS) Program. J Gastrointest Surg. 2017 - PubMed
-
- Recart A, Duchene D, White PF, Thomas T, Johnson DB, Cadeddu JA. Efficacy and safety of fast-track recovery strategy for patients undergoing laparoscopic nephrectomy. J Endourol. 2005;19(10):1165–1169. - PubMed
-
- Visioni A, Shah R, Gabriel E, Attwood K, Kukar M, Nurkin S. Enhanced Recovery After Surgery for Noncolorectal Surgery?: A Systematic Review and Meta-analysis of Major Abdominal Surgery. Ann Surg. 2017 - PubMed
-
- Fearon KC, Ljungqvist O, Von Meyenfeldt M, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr. 2005;24(3):466–477. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
