

Persistent inflammation, immunosuppression, and catabolism and the development of chronic critical illness after surgery
- PMID: 29807651
- PMCID: PMC6056337
- DOI: 10.1016/j.surg.2018.04.011
Persistent inflammation, immunosuppression, and catabolism and the development of chronic critical illness after surgery
Abstract
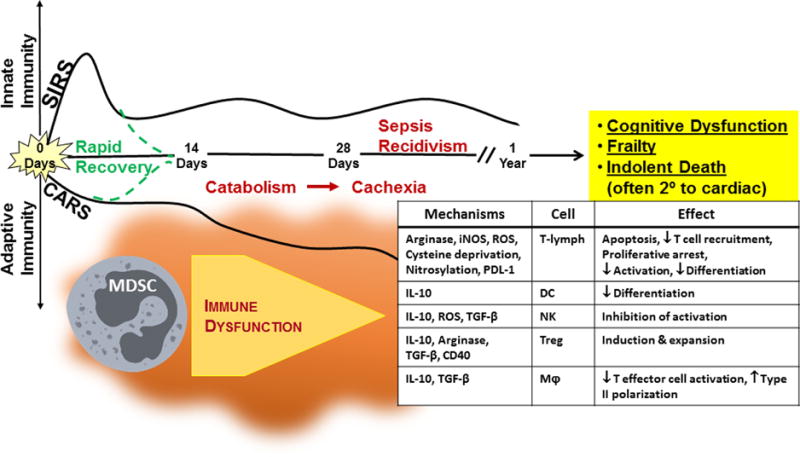
As early as the 1990s, chronic critical illness, a distinct syndrome of persistent high-acuity illness requiring management in the ICU, was reported under a variety of descriptive terms including the "neuropathy of critical illness," "myopathy of critical illness," "ICU-acquired weakness," and most recently "post-intensive care unit syndrome." The widespread implementation of targeted shock resuscitation, improved organ support modalities, and evidence-based protocolized ICU care has resulted in significantly decreased in-hospital mortality within surgical ICUs, specifically by reducing early multiple organ failure deaths. However, a new phenotype of multiple organ failure has now emerged with persistent but manageable organ dysfunction, high resource utilization, and discharge to prolonged care facilities. This new multiple organ failure phenotype is now clinically associated with the rapidly increasing incidence of chronic critical illness in critically ill surgery patients. Although the underlying pathophysiology driving chronic critical illness remains incompletely described, the persistent inflammation, immunosuppression, and catabolism syndrome has been proposed as a mechanistic framework in which to explain the increased incidence of chronic critical illness in surgical ICUs. The purpose of this review is to provide a historic perspective of the epidemiologic evolution of multiple organ failure into persistent inflammation, immunosuppression, and catabolism syndrome; describe the mechanism that drives and sustains chronic critical illness, and review the long-term outcomes of surgical patients who develop chronic critical illness.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest and Financial Disclosure Statement: No conflict of or competing interests has been declared.
Figures
References
-
- Moore FA, Moore EE. Evolving concepts in the pathogenesis of postinjury multiple organ failure. The Surgical clinics of North America. 1995;75(2):257–77. - PubMed
-
- Faist E, Baue AE, Dittmer H, Heberer G. Multiple organ failure in polytrauma patients. The Journal of trauma. 1983;23(9):775–87. - PubMed
-
- Moore FA, Sauaia A, Moore EE, Haenel JB, Burch JM, Lezotte DC. Postinjury multiple organ failure: a bimodal phenomenon. J Trauma. 1996;40(4):501–10. discussion 10-2. - PubMed
-
- Dewar DC, Tarrant SM, King KL, Balogh ZJ. Changes in the epidemiology and prediction of multiple-organ failure after injury. J Trauma Acute Care Surg. 2013;74(3):774–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
