

Evaluation of a community paramedicine health promotion and lifestyle risk assessment program for older adults who live in social housing: a cluster randomized trial
- PMID: 29807936
- PMCID: PMC5973885
- DOI: 10.1503/cmaj.170740
Evaluation of a community paramedicine health promotion and lifestyle risk assessment program for older adults who live in social housing: a cluster randomized trial
Abstract
Background: Low-income older adults who live in subsidized housing have higher mortality and morbidity. We aimed to determine if a community paramedicine program - in which paramedics provide health care services outside of the traditional emergency response - reduced the number of ambulance calls to subsidized housing for older adults.
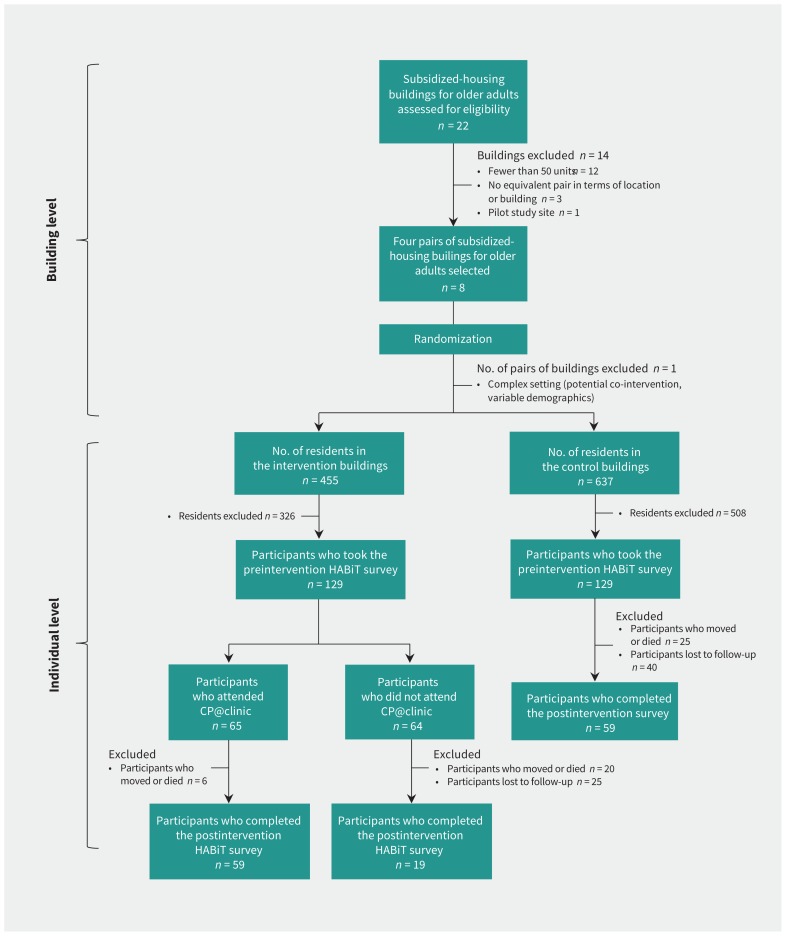
Methods: We conducted an open-label pragmatic cluster-randomized controlled trial (RCT) with parallel intervention and control groups in subsidized apartment buildings for older adults. We selected 6 buildings using predefined criteria, which we then randomly assigned to intervention (Community Paramedicine at Clinic [CP@clinic] for 1 yr) or control (usual health care) using computer-generated paired randomization. CP@clinic is a paramedic-led, community-based health promotion program to prevent diabetes, cardiovascular disease and falls for residents 55 years of age and older. The primary outcome was building-level mean monthly ambulance calls. Secondary outcomes were individual-level changes in blood pressure, health behaviours and risk of diabetes assessed using the Canadian Diabetes Risk Questionnaire. We analyzed the data using generalized estimating equations and hierarchical linear modelling.
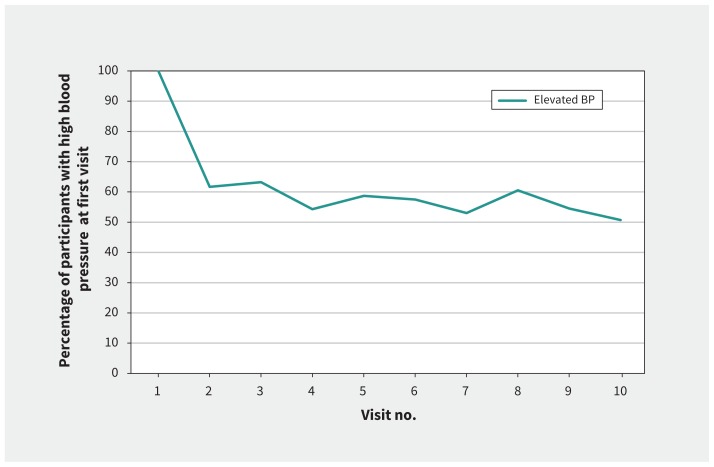
Results: The 3 intervention and 3 control buildings had 455 and 637 residents, respectively. Mean monthly ambulance calls in the intervention buildings (3.11 [standard deviation (SD) 1.30] calls per 100 units/mo) was significantly lower (-0.88, 95% confidence interval [CI] -0.45 to -1.30) than in control buildings (3.99 [SD 1.17] calls per 100 units/mo), when adjusted for baseline calls and building pairs. Survey participation was 28.4% (n = 129) and 20.3% (n = 129) in the intervention and control buildings, respectively. Residents living in the intervention buildings showed significant improvement compared with those living in control buildings in quality-adjusted life years (QALYs) (mean difference 0.09, 95% CI 0.01 to 0.17) and ability to perform usual activities (odds ratio 2.6, 95% CI 1.2 to 5.8). Those who received the intervention had a significant decrease in systolic (mean change 5.0, 95% CI 1.0 to 9.0) and diastolic (mean change 4.8, 95% CI 1.9 to 7.6) blood pressure.
Interpretation: A paramedic-led, community-based health promotion program (CP@clinic) significantly lowered the number of ambulance calls, improved QALYs and ability to perform usual activities, and lowered systolic blood pressure among older adults living in subsidized housing. Trial registration: Clinicaltrials.gov, no. NCT02152891.
© 2018 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
- CMAJ. 190:E636.
References
-
- Global status report on noncommunicable diseases 2010. Geneva: World Health Organization; 2011.
-
- Derlet RW, Richards JR. Overcrowding in the nation’s emergency departments: Complex causes and disturbing effects. Ann Emerg Med 2000;35:63–8. - PubMed
-
- Global health risks: mortality and burden of disease attributable to selected major risks. Geneva: World Health Organization Press; 2009.
-
- Chronic Disease Surveillance and Monitoring Division. Diabetes in Canada: facts and figures from a public health perspective. Ottawa: Public Health Agency of Canada; 2011.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous