

Quadrivalent human papillomavirus vaccination in girls and the risk of autoimmune disorders: the Ontario Grade 8 HPV Vaccine Cohort Study
- PMID: 29807937
- PMCID: PMC5973886
- DOI: 10.1503/cmaj.170871
Quadrivalent human papillomavirus vaccination in girls and the risk of autoimmune disorders: the Ontario Grade 8 HPV Vaccine Cohort Study
Abstract
Background: Despite demonstrated effectiveness in real-world settings, concerns persist regarding the safety of the quadrivalent human papillomavirus (HPV4) vaccine. We sought to assess the risk of autoimmune disorders following HPV4 vaccination among grade 8 girls eligible for Ontario's school-based HPV vaccination program.
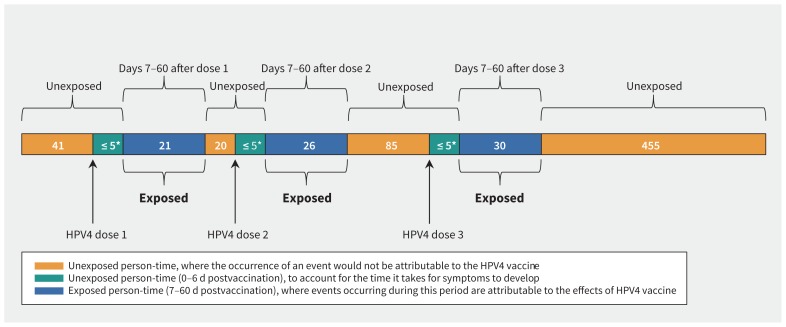
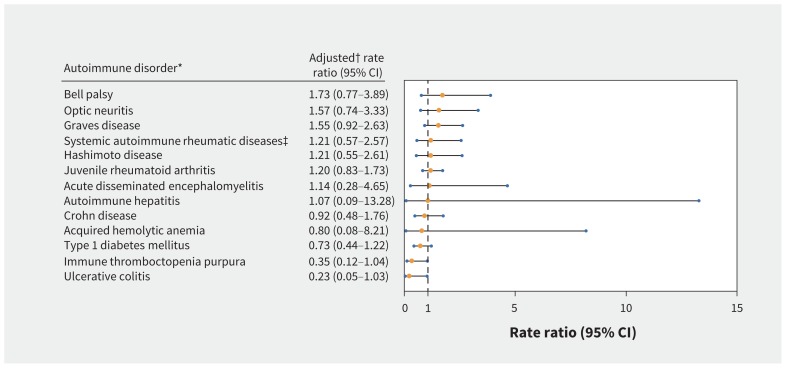
Methods: We undertook a population-based retrospective cohort study using Ontario's administrative health and vaccination databases from 2007 to 2013. The self-controlled case series method was used to compare the rate of a composite end point of autoimmune disorders diagnosed during days 7-60 post-vaccination ("exposed" follow-up) to that at any other time ("unexposed"). The analysis was repeated to assess the effect of a history of immune-mediated diseases and time since vaccination. We also conducted an exploratory analysis of individual autoimmune disorders. Rate ratios and 95% confidence intervals (CIs) were estimated using conditional Poisson regression, adjusted for age, seasonality, concomitant vaccinations and infections.
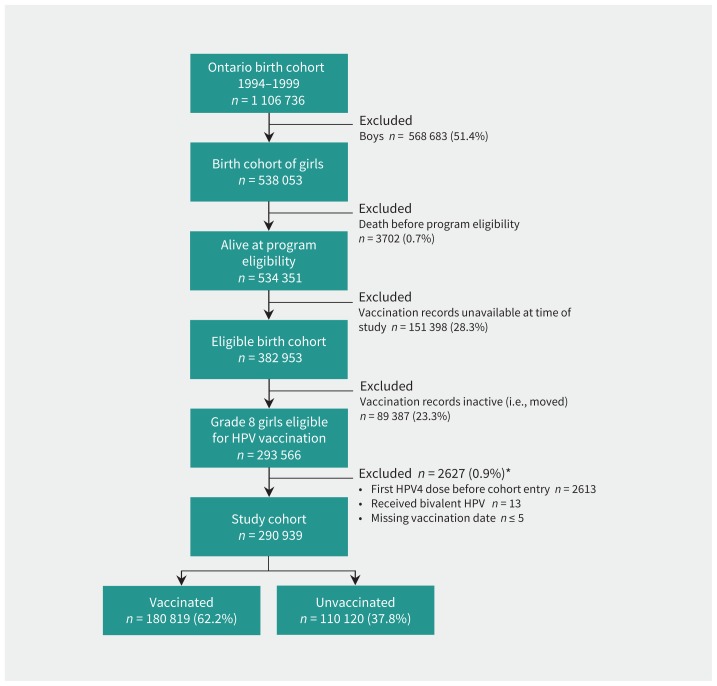
Results: The study cohort consisted of 290 939 girls aged 12-17 years who were eligible for vaccination between 2007 and 2013. There was no significant risk for developing an autoimmune disorder following HPV4 vaccination (n = 681; rate ratio 1.12, 95% CI 0.85-1.47), and the association was unchanged by a history of immune-mediated disorders and time since vaccination. Exploratory analyses of individual autoimmune disorders found no significant risks, including for Bell palsy (n = 65; rate ratio 1.73, 95% CI 0.77-3.89), optic neuritis (n = 67; rate ratio 1.57, 95% CI 0.74-3.33) and Graves disease (n = 47; rate ratio 1.55, 95% CI 0.92-2.63).
Interpretation: We did not observe an increased risk of autoimmune disorders following HPV4 vaccination among teenaged girls. These findings should reassure parents and health care providers.
© 2018 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Leah Smith is now employed by the Canadian Cancer Society, a charitable organization that promotes HPV vaccination and has received funds from Merck. However, this study was completed before Dr. Smith’s employment at the Canadian Cancer Society. Anne Ellis reports funding from ALK-Abelló, AstraZeneca, Bayer, Merck, Novartis, Pediapharm, Pfizer, Sanofi, Takeda and SunPharma. Linda Lévesque is now employed by Sanofi Pasteur, a global vaccine manufacturer; however, this study was completed before her employment at Sanofi Pasteur. No other competing interests were declared.
Figures
References
-
- Trottier H, Franco E. The epidemiology of genital human papillomavirus infection. Vaccine 2006;24(Suppl 1):S1–15. - PubMed
-
- Baseman JG, Koutsky L. The epidemiology of human papillomavirus infections. J Clin Virol 2005;32:(Suppl 1):S16–24. - PubMed
-
- Tota JE, Chevarie-Davis M, Richardson L, et al. Epidemiology and burden of HPV infection and related diseases: implications for prevention strategies. Prev Med 2011;53:(Suppl 1):S12–21. - PubMed
-
- Smith LM, Strumpf EC, Kaufman JS, et al. The early benefits of human papillomavirus vaccination on cervical dysplasia and anogenital warts. Pediatrics 2015;135:e1131-40 10.1542/peds.2014-2961. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical