

Myelitis due to Coccidioidomycosis in an Immunocompetent Patient
- PMID: 29808132
- PMCID: PMC5902110
- DOI: 10.1155/2018/2176269
Myelitis due to Coccidioidomycosis in an Immunocompetent Patient
Abstract
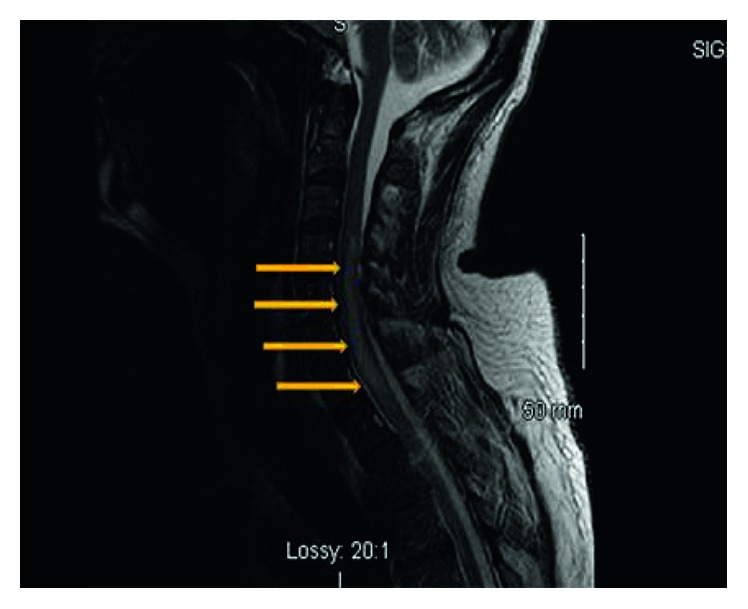
Myelitis of the spinal cord is an uncommon presentation of disseminated coccidioidomycosis. Most infected patients present subclinically, but patients, especially those who are immunocompromised, may progress to disseminated disease. We present a 50-year-old immunocompetent patient with no significant past medical history exhibiting symptoms of altered mental status, dizziness, headache, nausea, and quadriplegia. Upon investigation with lumbar puncture, cerebrospinal fluid (CSF) culture, and coccidioidal antibody studies, the patient was found to have acute coccidioidomycosis. Magnetic resonance imaging (MRI) of the brain demonstrated meningeal enhancements suggestive of meningitis, and further MRI study of the cervical spine revealed myelitis. Treatment with IV fluconazole for 2 weeks and IV voriconazole therapy over 3 weeks yielded limited improvement. The presentation of myelitis due to coccidioidomycosis infection is very rare and has infrequently reported in the literature. Awareness of this potentially fatal complication in immunocompetent patients can aid in faster recognition and treatment.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
