

Outcome in patients perceived as receiving excessive care across different ethical climates: a prospective study in 68 intensive care units in Europe and the USA
- PMID: 29808345
- PMCID: PMC6061457
- DOI: 10.1007/s00134-018-5231-8
Outcome in patients perceived as receiving excessive care across different ethical climates: a prospective study in 68 intensive care units in Europe and the USA
Abstract
Purpose: Whether the quality of the ethical climate in the intensive care unit (ICU) improves the identification of patients receiving excessive care and affects patient outcomes is unknown.
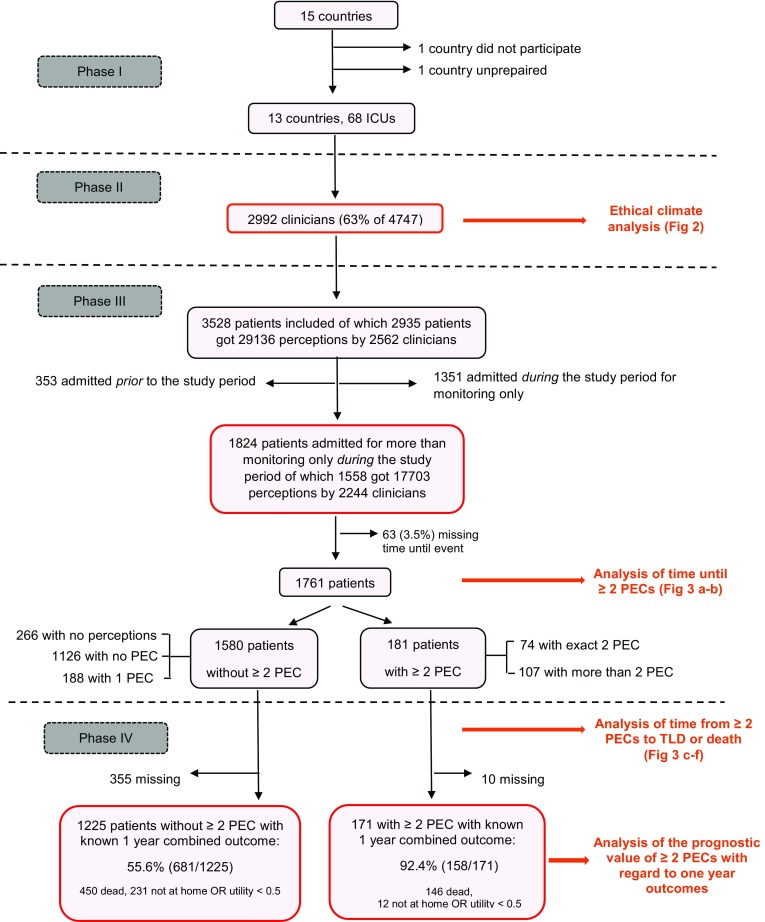
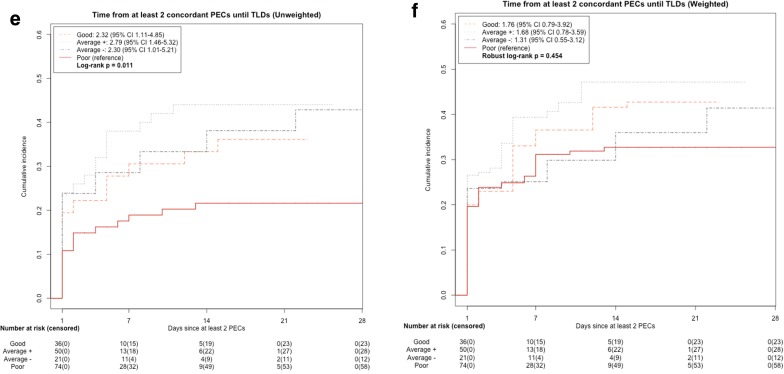
Methods: In this prospective observational study, perceptions of excessive care (PECs) by clinicians working in 68 ICUs in Europe and the USA were collected daily during a 28-day period. The quality of the ethical climate in the ICUs was assessed via a validated questionnaire. We compared the combined endpoint (death, not at home or poor quality of life at 1 year) of patients with PECs and the time from PECs until written treatment-limitation decisions (TLDs) and death across the four climates defined via cluster analysis.
Results: Of the 4747 eligible clinicians, 2992 (63%) evaluated the ethical climate in their ICU. Of the 321 and 623 patients not admitted for monitoring only in ICUs with a good (n = 12, 18%) and poor (n = 24, 35%) climate, 36 (11%) and 74 (12%), respectively were identified with PECs by at least two clinicians. Of the 35 and 71 identified patients with an available combined endpoint, 100% (95% CI 90.0-1.00) and 85.9% (75.4-92.0) (P = 0.02) attained that endpoint. The risk of death (HR 1.88, 95% CI 1.20-2.92) or receiving a written TLD (HR 2.32, CI 1.11-4.85) in patients with PECs by at least two clinicians was higher in ICUs with a good climate than in those with a poor one. The differences between ICUs with an average climate, with (n = 12, 18%) or without (n = 20, 29%) nursing involvement at the end of life, and ICUs with a poor climate were less obvious but still in favour of the former.
Conclusion: Enhancing the quality of the ethical climate in the ICU may improve both the identification of patients receiving excessive care and the decision-making process at the end of life.
Keywords: Decision-making; Ethical climate; Interdisciplinary collaboration; Patient outcomes; Perceived excessive care; Treatment-limitation decisions.
Conflict of interest statement
DB reports grants from Gilead, Astellas, Fisher-Paykel, Baxter, Alexion and Fresenius Kabi outside the submitted work. KR reports honoraria from Alexion, outside the submitted work. MD reports grant from MSD and Jazz Pharma, personal fees from Astellas and Bristol-Myers Squibb, and non-financial support from Astellas, Bristol-Myers Squibb, Astute Medical, and Sanofi Aventis. EA reports grants and personal fees from Gilead, Alexion, MSD, Cubist and personal fees from Baxter, outside the submitted work. All other authors have no conflict of interest to report.
Figures


References
-
- Teno JM, Gozalo PL, Bynum JPW, Leland NE, Miller SC, Morden NE, Scupp T, Goodman DC, Mor V. Change in end-of-life care for medicare beneficiaries. Site of death, place of care, and health care transtitions in 2001 2005, and 2009. JAMA. 2013;309:470–477. doi: 10.1001/jama.2012.207624. - DOI - PMC - PubMed
-
- Wang CY, Calfee CS, Paul DW, Janz DR, May AK, Zhuo H, Bernard GR, Matthay MA, Ware LB, Neudoerffer Kangelaris K. One-year mortality and predictors of death among hospital survivors of acute respiratory distress syndrome. Intensive Care Med. 2014;40:388–396. doi: 10.1007/s00134-013-3186-3. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
