

Growth patterns and cerebroplacental hemodynamics in fetuses with congenital heart disease
- PMID: 29808509
- PMCID: PMC6593432
- DOI: 10.1002/uog.19102
Growth patterns and cerebroplacental hemodynamics in fetuses with congenital heart disease
Abstract
Objectives: Congenital heart disease (CHD) has been associated with reduced fetal head circumference (HC), although the underlying pathophysiology remains undetermined. We aimed to define trends in fetal growth and cerebroplacental Doppler flow, and to investigate their relationship, in fetuses with CHD.
Methods: This was a retrospective study in two fetal medicine units in The Netherlands. We included all fetuses with CHD in whom Doppler flow patterns (middle cerebral artery (MCA) pulsatility index (PI), umbilical artery (UA) PI and cerebroplacental ratio (CPR)) and biometry (HC and abdominal circumference (AC)) had been measured serially after 19 weeks' gestation between January 2010 and November 2016. Fetuses were categorized into three groups based on the expected cerebral arterial oxygen saturation of their particular type of CHD: normal; mild to moderately reduced; severely reduced. Trends over time in Z-scores were analyzed using a linear mixed-effects model.
Results: A total of 181 fetuses fulfilled the inclusion criteria. Expected cerebral arterial oxygen saturation in CHD was classified as normal in 44 cases, mild to moderately reduced in 84 and severely reduced in 53. In the cohort overall, average trends over time were significant for both HC and AC Z-scores. HC Z-scores showed a tendency to decrease until 23 weeks, then to increase until 33 weeks, followed by another decrease in the late third trimester. AC Z-scores increased progressively with advancing gestation. MCA-PI and UA-PI Z-scores showed significant trends throughout pregnancy, but CPR Z-scores did not. There were no associations between expected cerebral arterial oxygen saturation and fetal growth. Average trends in MCA-PI Z-scores were significantly different between the three subgroups, whereas those in UA-PI Z-scores and in CPR Z-scores were similar between the subgroups. There was no significant association between MCA-PI and HC Z-scores.
Conclusions: Fetal biometry and Doppler flow patterns are within normal range in fetuses with CHD, but show trends over time. Head growth in fetuses with CHD is not associated with cerebral blood flow pattern or placental function and HC is not influenced by the cerebral arterial oxygen saturation. © 2018 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of the International Society of Ultrasound in Obstetrics and Gynecology.
Keywords: Doppler flow patterns; congenital heart disease; growth; head circumference; oxygenation.
© 2018 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of the International Society of Ultrasound in Obstetrics and Gynecology.
Figures
 ), mild to moderately reduced (
), mild to moderately reduced ( ) or severely reduced (
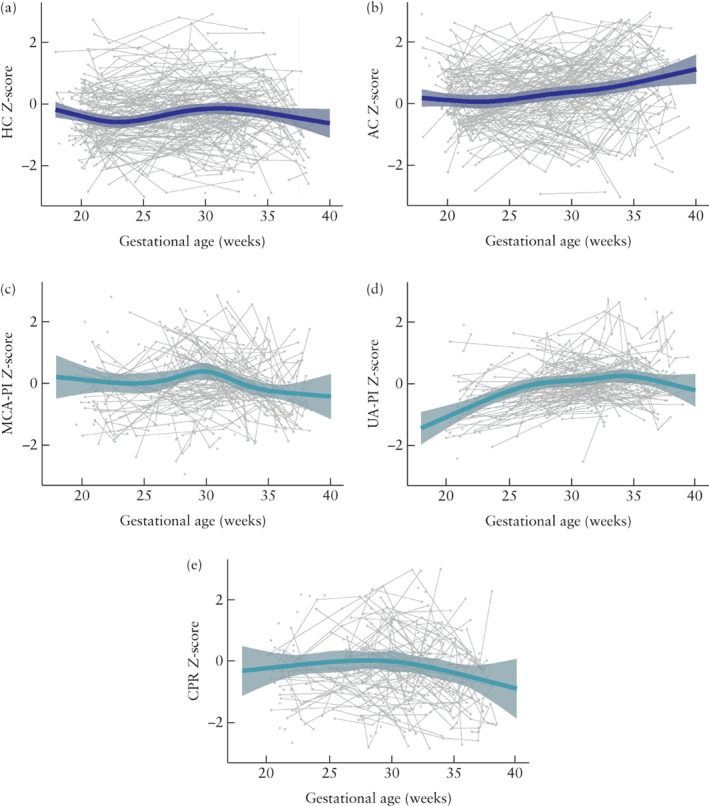
) or severely reduced ( ). 95% CIs of fitted model are shaded gray. (a) Head circumference (HC); (b) abdominal circumference (AC); (c) middle cerebral artery pulsatility index (MCA‐PI); (d) umbilical artery pulsatility index (UA‐PI); (e) cerebroplacental ratio (CPR).
). 95% CIs of fitted model are shaded gray. (a) Head circumference (HC); (b) abdominal circumference (AC); (c) middle cerebral artery pulsatility index (MCA‐PI); (d) umbilical artery pulsatility index (UA‐PI); (e) cerebroplacental ratio (CPR).
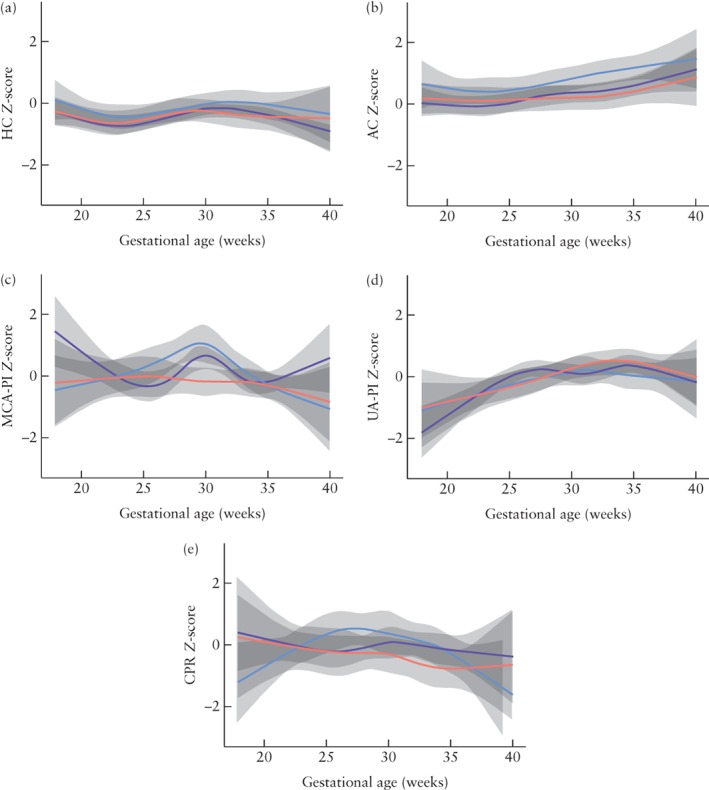
 ), mild to moderately reduced (
), mild to moderately reduced ( ) or severely reduced (
) or severely reduced ( ) cerebral arterial oxygen saturation. 95% CIs of fitted model are shaded gray for total cohort only; those for CHD subgoups were broad and overlapping.
) cerebral arterial oxygen saturation. 95% CIs of fitted model are shaded gray for total cohort only; those for CHD subgoups were broad and overlapping.References
-
- Ruiz A, Cruz‐Lemini M, Masoller N, Sanz‐Cortes M, Ferrer Q, Ribera I, Martínez JM, Crispi F, Arévalo S, Gómez O, Pérez‐Hoyos S, Carreras E, Gratacós E, Llurba E. Longitudinal changes in fetal biometry and cerebroplacental hemodynamics in fetuses with congenital heart disease. Ultrasound Obstet Gynecol 2017; 49: 379–386. - PubMed
-
- Hahn E, Szwast A, Cnota J, Levine JC, Fifer CG, Jaeggi E, Andrews H, Williams IA. Association between fetal growth, cerebral blood flow and neurodevelopmental outcome in univentricular fetuses. Ultrasound Obstet Gynecol 2016; 47: 460–465. - PubMed
-
- Zeng S, Zhou QC, Zhou JW, Li M, Long C, Peng QH. Volume of intracranial structures on three‐dimensional ultrasound in fetuses with congenital heart disease. Ultrasound Obstet Gynecol 2015; 46: 174–181. - PubMed
-
- Masoller N, Martinez JM, Gomez O, Bennasar M, Crispi F, Sanz‐Cortés M, Egaña‐Ugrinovic G, Bartrons J, Puerto B, Gratacós E. Evidence of second‐trimester changes in head biometry and brain perfusion in fetuses with congenital heart disease. Ultrasound Obstet Gynecol 2014; 44: 182–187. - PubMed
-
- Yamamoto Y, Khoo NS, Brooks PA, Savard W, Hirose A, Hornberger LK. Severe left heart obstruction with retrograde arch flow influences fetal cerebral and placental blood flow. Ultrasound Obstet Gynecol 2013; 42: 294–299. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
