

Identifying Patients for Whom Lung Cancer Screening Is Preference-Sensitive: A Microsimulation Study
- PMID: 29809244
- PMCID: PMC6033668
- DOI: 10.7326/M17-2561
Identifying Patients for Whom Lung Cancer Screening Is Preference-Sensitive: A Microsimulation Study
Abstract
Background: Many health systems are exploring how to implement low-dose computed tomography (LDCT) screening programs that are effective and patient-centered.
Objective: To examine factors that influence when LDCT screening is preference-sensitive.
Design: State-transition microsimulation model.
Data sources: Two large randomized trials, published decision analyses, and the SEER (Surveillance, Epidemiology, and End Results) cancer registry.
Target population: U.S.-representative sample of simulated patients meeting current U.S. Preventive Services Task Force criteria for screening eligibility.
Time horizon: Lifetime.
Perspective: Individual.
Intervention: LDCT screening annually for 3 years.
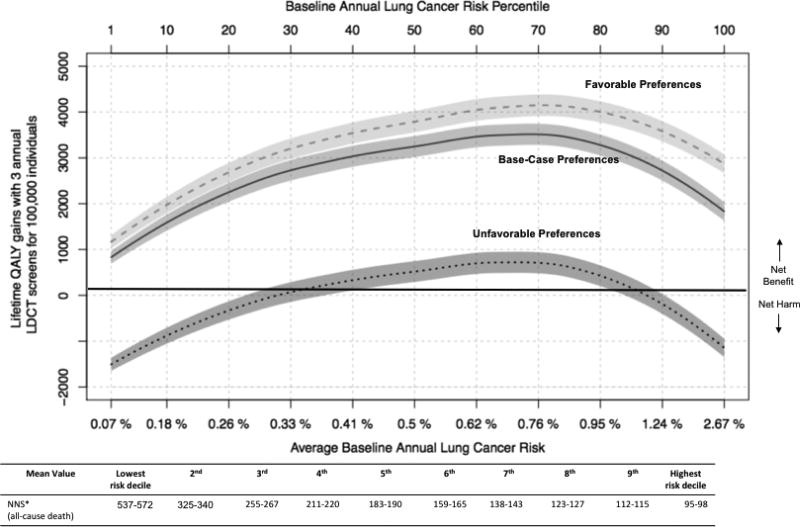
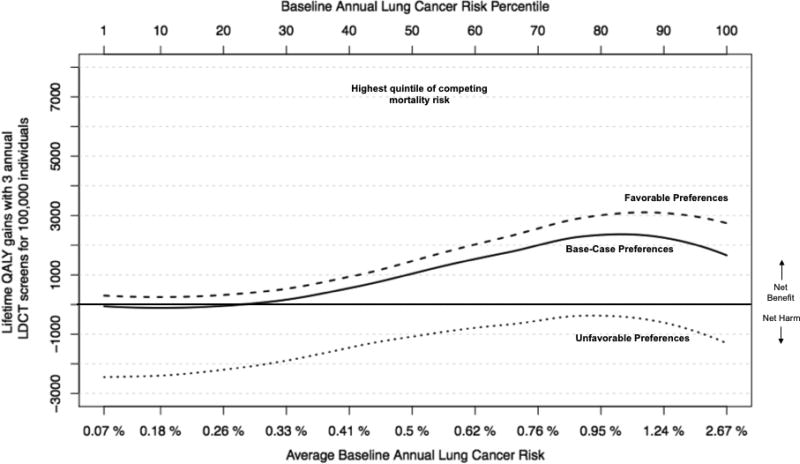
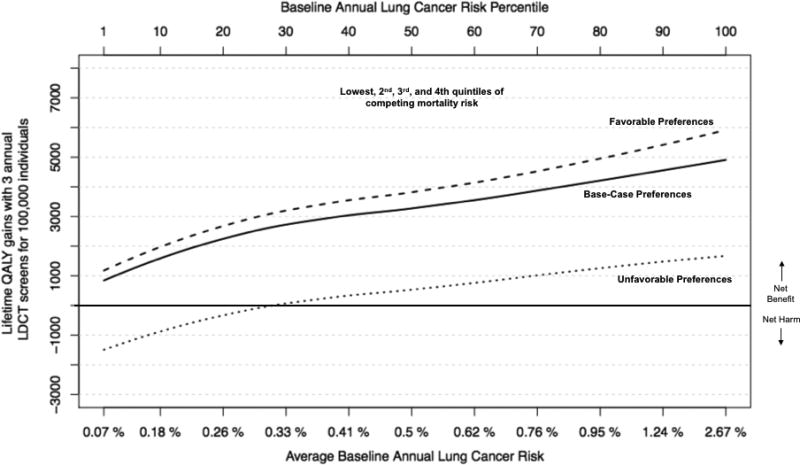
Outcome measures: Lifetime quality-adjusted life-year gains and reduction in lung cancer mortality. To examine the effect of preferences on net benefit, disutilities (the "degree of dislike") quantifying the burden of screening and follow-up were varied across a likely range. The effect of varying the rate of false-positive screening results and overdiagnosis associated with screening was also examined.
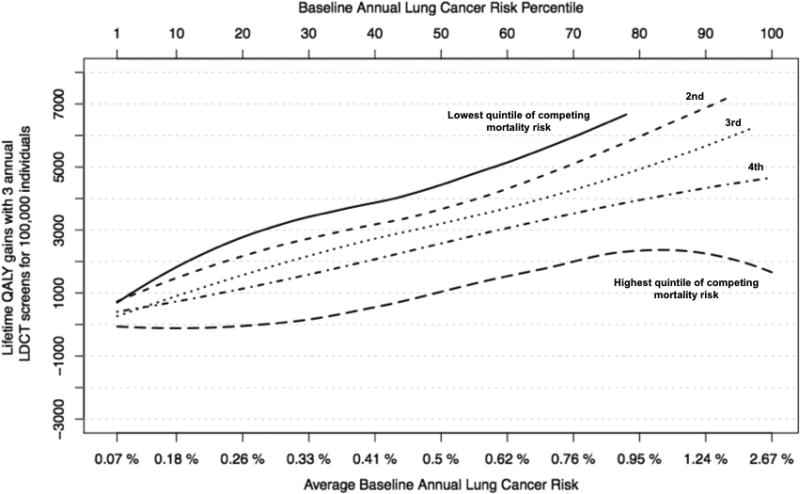
Results of base-case analysis: Moderate differences in preferences about the downsides of LDCT screening influenced whether screening was appropriate for eligible persons with annual lung cancer risk less than 0.3% or life expectancy less than 10.5 years. For higher-risk eligible persons with longer life expectancy (roughly 50% of the study population), the benefits of LDCT screening overcame even highly negative views about screening and its downsides.
Results of sensitivity analysis: Rates of false-positive findings and overdiagnosed lung cancer were not highly influential.
Limitation: The quantitative thresholds that were identified may vary depending on the structure of the microsimulation model.
Conclusion: Identifying circumstances in which LDCT screening is more versus less preference-sensitive may help clinicians personalize their screening discussions, tailoring to both preferences and clinical benefit.
Primary funding source: None.
Figures
Comment in
-
Precision Screening for Lung Cancer: Risk-Based but Not Always Preference-Sensitive?Ann Intern Med. 2018 Jul 3;169(1):52-53. doi: 10.7326/M18-1350. Epub 2018 May 29. Ann Intern Med. 2018. PMID: 29809245 No abstract available.
-
The impact of patients' preferences on the decision of low-dose computed tomography lung cancer screening.Transl Lung Cancer Res. 2018 Sep;7(Suppl 3):S236-S238. doi: 10.21037/tlcr.2018.08.17. Transl Lung Cancer Res. 2018. PMID: 30393611 Free PMC article. No abstract available.
-
Identifying Patients for Whom Lung Cancer Screening Is Preference-Sensitive.Ann Intern Med. 2018 Dec 4;169(11):822-823. doi: 10.7326/L18-0555. Ann Intern Med. 2018. PMID: 30508438 No abstract available.
-
Identifying Patients for Whom Lung Cancer Screening Is Preference-Sensitive.Ann Intern Med. 2018 Dec 4;169(11):823. doi: 10.7326/L18-0556. Ann Intern Med. 2018. PMID: 30508439 No abstract available.
References
-
- [cited 2018 Mar 11];Cancer of the Lung and Bronchus - SEER Stat Fact Sheets [Internet] Available from: http://seer.cancer.gov/statfacts/html/lungb.html.
-
- Kinsinger LS, Anderson C, Kim J, Larson M, Chan SH, King HA, et al. Implementation of Lung Cancer Screening in the Veterans Health Administration. JAMA Intern Med. 2017 Mar 1;177(3):399–406. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials