

Symptomatic Zika Virus Infection in Infants, Children, and Adolescents Living in Puerto Rico
- PMID: 29813148
- PMCID: PMC6137503
- DOI: 10.1001/jamapediatrics.2018.0870
Symptomatic Zika Virus Infection in Infants, Children, and Adolescents Living in Puerto Rico
Abstract
Importance: Little information is available regarding Zika virus (ZIKV) infection in children.
Objective: To describe patients younger than 18 years who were infected with ZIKV and were enrolled in the Sentinel Enhanced Dengue and Acute Febrile Illness Surveillance System (SEDSS).
Design, setting, and participants: Children infected with ZIKV with 7 or fewer days of fever or emancipated minors aged 14 to 17 years with a generalized maculopapular rash, arthritis or arthralgia, or nonpurulent conjunctivitis were eligible for enrollment on or before December 31, 2016, in Puerto Rico. Patients were evaluated using ZIKV polymerase chain reaction testing at 7 or fewer days after the onset of symptoms. Available ZIKV polymerase chain reaction-positive specimens were evaluated to determine viral loads.
Exposures: Confirmed polymerase chain reaction-positive ZIKV infection.
Main outcomes and measures: Clinical characteristics and viral loads of symptomatic children with confirmed ZIKV infection.
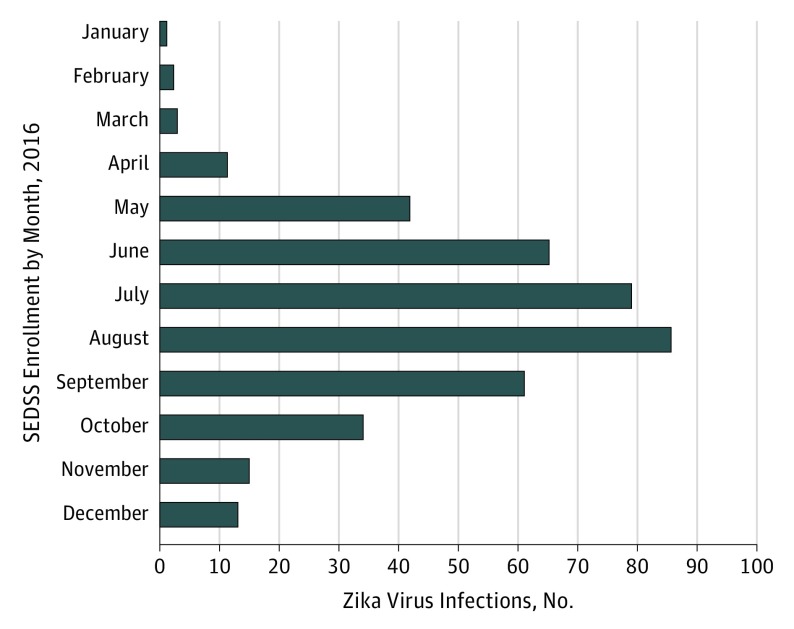
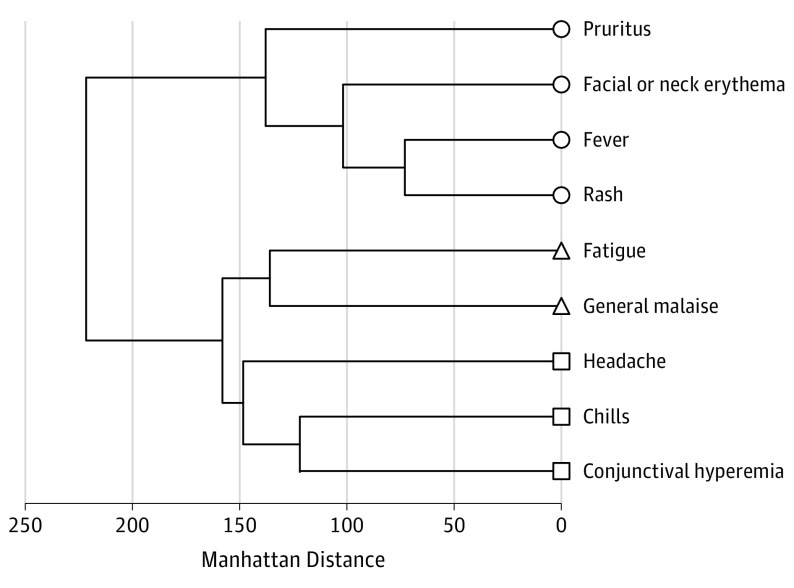
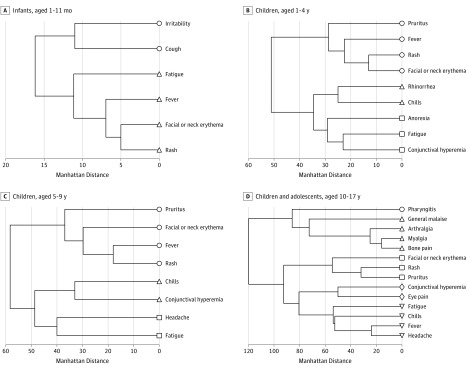
Results: Of 7191 children enrolled in SEDSS on or before December 31, 2016, only those with confirmed ZIKV infection (351 participants) were included in this study. Participants who had confirmed ZIKV infection included 25 infants (7.1%), 69 children (19.7%) aged 1 to 4 years, 95 (27.1%) aged 5 to 9 years, and 162 (46.1%) aged 10 to 17 years. Among these, 260 patients (74.1%) presented for evaluation of ZIKV infection at fewer than 3 days after the onset of symptoms, 340 (96.9%) were discharged to home after evaluation, and 349 (99.4%) had fever, 280 (79.8%) had a rash, 243 (69.2%) had facial or neck erythema, 234 (66.7%) had fatigue, 223 (63.5%) had headache, 212 (60.4%) had chills, 206 (58.7%) had pruritus, and 204 (58.1%) had conjunctival hyperemia. Of 480 specimens collected (317 serum and 163 urine specimens) from 349 children, the median number of days after the onset of symptoms was lower for children who had serum specimens (1 day [interquartile range (IQR), 1-2 days]) than for children who had urine specimens (2 [1-3] days) (P < .001). Of 131 children who had both serum and urine specimens collected on the same day, the median viral load was higher in serum than in urine (median [IQR], 23 098 [8784-88 242] copies/mL for serum vs 9966 [2815-52 774] copies/mL for urine; P = .02). When a single serum sample from each of 317 patients was analyzed, there were no statistically significant differences in median viral loads according to age, sex, or disposition. However, the median serum viral load varied significantly according to the number of days after the onset of symptoms (0 days, 106 778 [IQR, 9772-1 571 718] copies/mL; 1 day, 46 299 [10 663-255 030] copies/mL; 2 days, 20 678 [8763-42 458] copies/mL; and ≥3 days, 15 901 [5135-49 248] copies/mL; P = .001).
Conclusions and relevance: This study represents the largest study to date of ZIKV infection in the pediatric population. Most children infected with ZIKV had fever, rash, and conjunctival hyperemia. The children usually presented for evaluation at fewer than 3 days after the onset of symptoms. Viral loads for ZIKV were higher in serum vs urine specimens. Median viral loads in serum specimens differed significantly according to the number of days after the onset of symptoms.
Conflict of interest statement
Figures
Comment in
-
Uncovering the Spectrum of Postnatal Zika Infection in Children.JAMA Pediatr. 2018 Jul 1;172(7):624-625. doi: 10.1001/jamapediatrics.2018.0921. JAMA Pediatr. 2018. PMID: 29813163 No abstract available.
References
-
- Simmonds P, Becher P, Collet MS, et al. Flaviviridae In: King AMQ, Adams MJ, Cartens EB, Lefkowitz EJ, eds. Virus Taxonomy: Ninth Report of the International Committee on Taxonomy of Viruses. San Diego, CA: Academic Press Elsevier; 2011:1008-1020.
-
- Marchette NJ, Garcia R, Rudnick A. Isolation of Zika virus from Aedes aegypti mosquitoes in Malaysia. Am J Trop Med Hyg. 1969;18(3):411-415. - PubMed
-
- Martines RB, Bhatnagar J, Keating MK, et al. Notes from the field: evidence of Zika virus infection in brain and placental tissues from two congenitally infected newborns and two fetal losses—Brazil, 2015. MMWR Morb Mortal Wkly Rep. 2016;65(6):159-160. - PubMed
-
- Martines RB, Bhatnagar J, de Oliveira Ramos AM, et al. Pathology of congenital Zika syndrome in Brazil. Lancet. 2016;388(10047):898-904. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
