

Horizontal gaze palsy with progressive scoliosis: a case report with magnetic resonance tractography and electrophysiological study
- PMID: 29843650
- PMCID: PMC5972445
- DOI: 10.1186/s12883-018-1081-9
Horizontal gaze palsy with progressive scoliosis: a case report with magnetic resonance tractography and electrophysiological study
Abstract
Background: Horizontal gaze palsy with progressive scoliosis (HGPPS) is a rare autosomal recessive congenital anomaly characterized by horizontal gaze limitation and progressive scoliosis. We investigated the underlying pathogenesis by incorporating diffusion tensor imaging and an electrophysiological study.
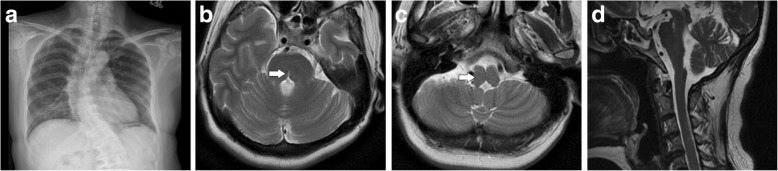
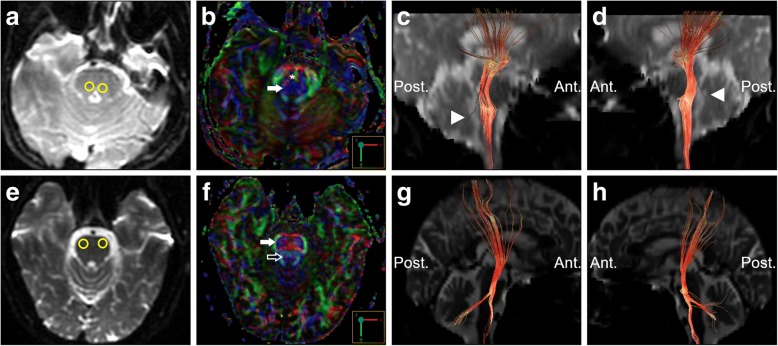
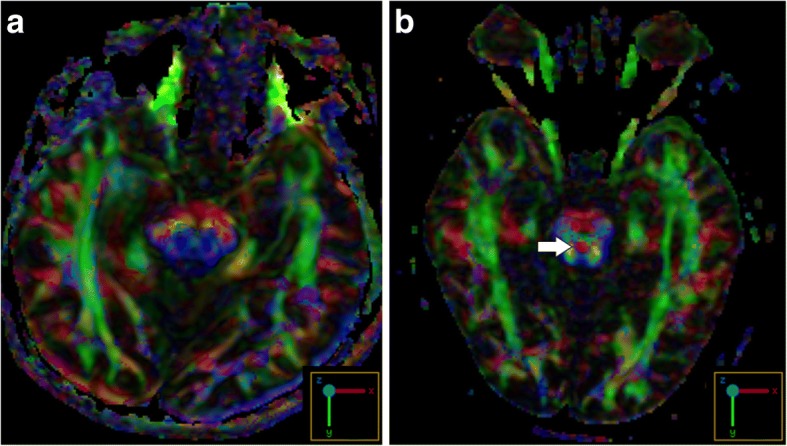
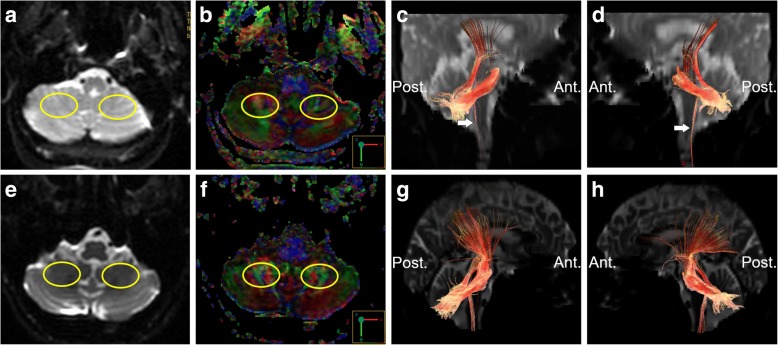
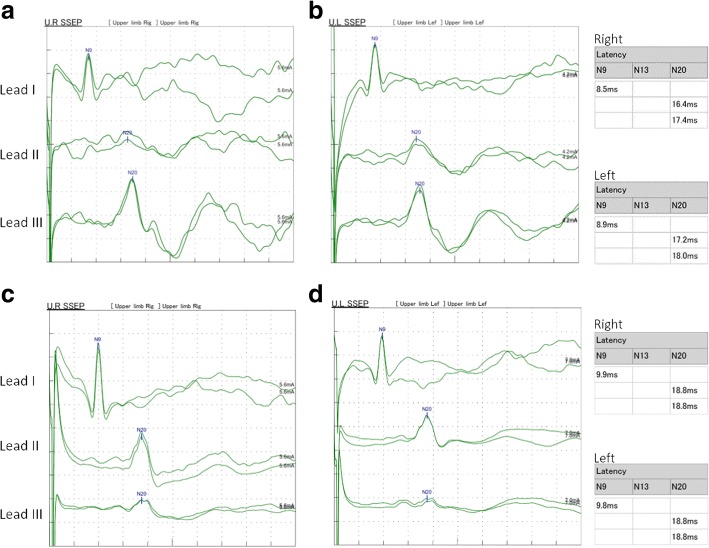
Case presentation: A 55-year-old female patient presented to our clinic due to a chronic history of eye movement limitation since childhood. Her eye problem was followed by a progressive scoliotic change in her torso during junior high school. Neurological examinations revealed remarkable conjugate horizontal but not vertical gaze palsy. Her pupils were isocoric, with a prompt response to light reflex and convergence. Her vision, including visual acuity and field, were normal. No pathological signs of muscle tone, muscle power, deep tendon reflex or coordination were revealed. There was no associated family history, and no diseases involving other systems were noted. On reviewing her past medical history, X-rays revealed scoliotic changes of her thoracic and lumbar spine. Brain magnetic resonance imaging showed a midline cleavage at the tegmentum (split pons sign) and butterfly configuration of the medulla, consistent with HGPPS. Color-coded diffusion tensor imaging in our patient revealed absence of decussation of the superior cerebellar peduncle. In tractography, the pontocerebellar tracts and fibers within the inferior cerebellar peduncle, deemed to be primarily dorsal spinocerebellar and vestibulocerebellar tracts, appeared to be agenetic. The tegmentum was compromised secondary to dorsal displacement of the corticospinal tracts. Of note, the bilateral corticospinal tracts remained uncrossed at the level presumed to be the pyramidal decussation. A somatosensory evoked potential study also revealed predominantly ipsilateral cortical sensory responses.
Conclusions: Our study confirmed that a compromised tegmentum secondary to dorsal displacement of the corticospinal tracts and poorly-developed afferent fibers within the pontocerebellar tracts and inferior cerebellar peduncle to be the main neuroanatomical anomalies responsible for the clinical presentations of HGPPS. In addition, the uncrossed nature of the majority of pyramidal and proprioceptive sensory systems was confirmed.
Keywords: Diffusion tensor imaging; Horizontal gaze palsy with progressive scoliosis; Magnetic resonance imaging; Somatosensory evoked potential; Split pons sign; Tractography.
Conflict of interest statement
Ethics approval and consent to participate
The authors declare that ethics approval was not required for this case report.
Consent for publication
Written informed consent was obtained from the patient and the healthy control for publication in this Case Report and any accompanying images. A copy of the written consent form is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
