

Is telephone health coaching a useful population health strategy for supporting older people with multimorbidity? An evaluation of reach, effectiveness and cost-effectiveness using a 'trial within a cohort'
- PMID: 29843795
- PMCID: PMC5975389
- DOI: 10.1186/s12916-018-1051-5
Is telephone health coaching a useful population health strategy for supporting older people with multimorbidity? An evaluation of reach, effectiveness and cost-effectiveness using a 'trial within a cohort'
Abstract
Background: Innovative ways of delivering care are needed to improve outcomes for older people with multimorbidity. Health coaching involves 'a regular series of phone calls between patient and health professional to provide support and encouragement to promote healthy behaviours'. This intervention is promising, but evidence is insufficient to support a wider role in multimorbidity care. We evaluated health coaching in older people with multimorbidity.
Methods: We used the innovative 'Trials within Cohorts' design. A cohort was recruited, and a trial was conducted using a 'patient-centred' consent model. A randomly selected group within the cohort were offered the intervention and were analysed as the intervention group whether they accepted the offer or not. The intervention sought to improve the skills of patients with multimorbidity to deal with a range of long-term conditions, through health coaching, social prescribing and low-intensity support for low mood.
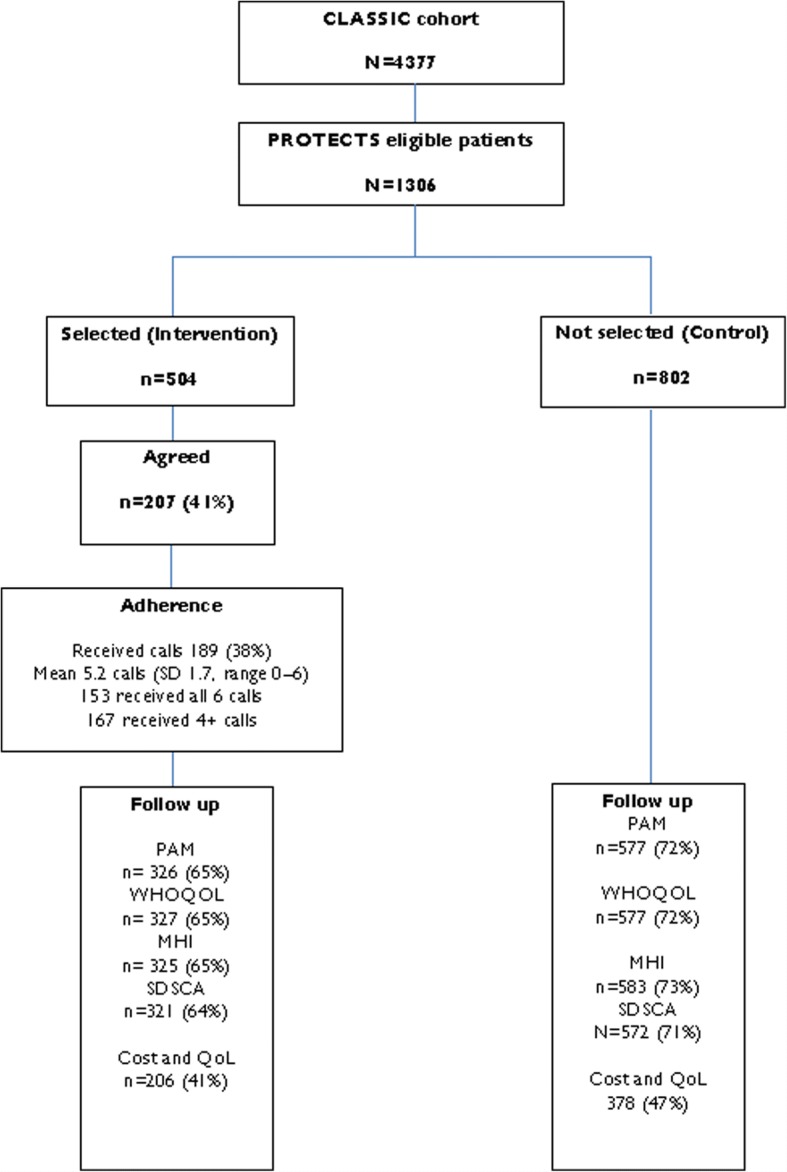
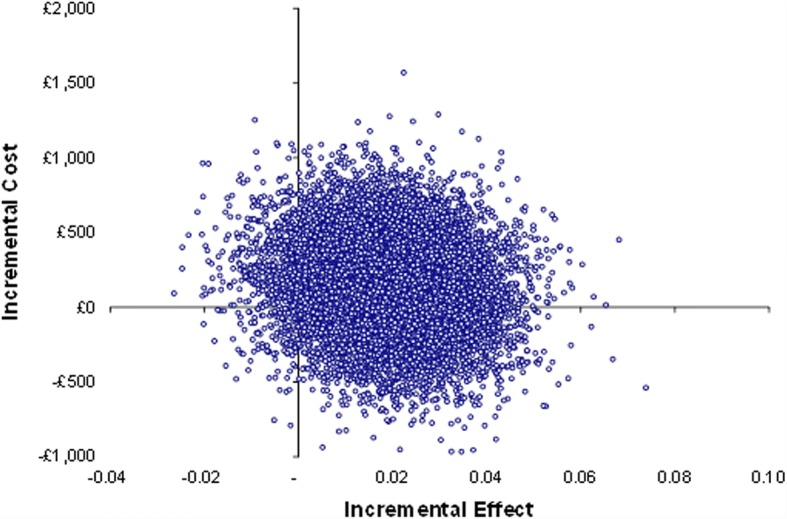
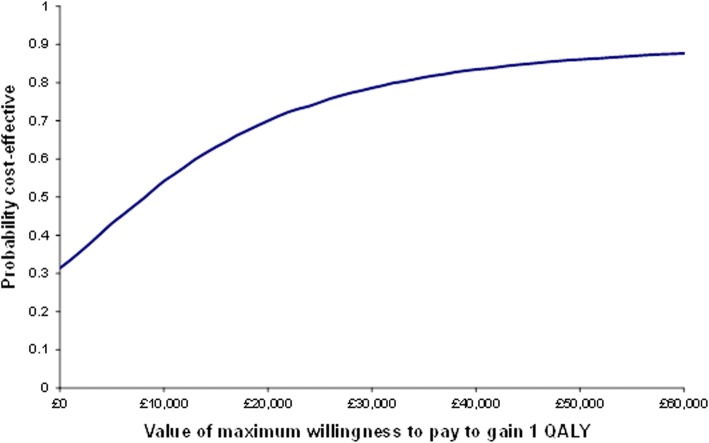
Results: We recruited 4377 older people, and 1306 met the eligibility criteria (two or more long-term conditions and moderate 'patient activation'). We selected 504 for health coaching, and 41% consented. More than 80% of consenters received the defined 'dose' of 4+ sessions. In an intention-to-treat analysis, those selected for health coaching did not improve on any outcome (patient activation, quality of life, depression or self-care) compared to usual care. We examined health care utilisation using hospital administrative and self-report data. Patients selected for health coaching demonstrated lower levels of emergency care use, but an increase in the use of planned services and higher overall costs, as well as a quality-adjusted life year (QALY) gain. The incremental cost per QALY was £8049, with a 70-79% probability of being cost-effective at conventional levels of willingness to pay.
Conclusions: Health coaching did not lead to significant benefits on the primary measures of patient-reported outcome. This is likely related to relatively low levels of uptake amongst those selected for the intervention. Demonstrating effectiveness in this design is challenging, as it estimates the effect of being selected for treatment, regardless of whether treatment is adopted. We argue that the treatment effect estimated is appropriate for health coaching, a proactive model relevant to many patients in the community, not just those seeking care.
Trial registration: International Standard Randomised Controlled Trial Number ( ISRCTN12286422 ).
Keywords: depression; health coaching; multimorbidity; older adults.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the National Research Ethics Service Committee North West–Lancaster (reference number 14/NW/0206). All participants consented to join the cohort study (CLASSIC), with those selected for the intervention providing consent for the trial.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Boyd CM, Fortin M. Future of multimorbidity research: how should understanding of multimorbidity inform health system design? Public Health Rev. 2010;32(2):451–474. doi: 10.1007/BF03391611. - DOI
-
- Coventry P, Fisher L, Kenning C, Bee P, Bower P. Capacity, responsibility, and motivation: a critical qualitative evaluation of patient and practitioner views about barriers to self-management in people with multimorbidity. BMC Health Serv Res. 2014;14:536. doi: 10.1186/s12913-014-0536-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
