

Adaptive Immune Responses in Hepatitis A Virus and Hepatitis E Virus Infections
- PMID: 29844218
- PMCID: PMC6531370
- DOI: 10.1101/cshperspect.a033472
Adaptive Immune Responses in Hepatitis A Virus and Hepatitis E Virus Infections
Abstract
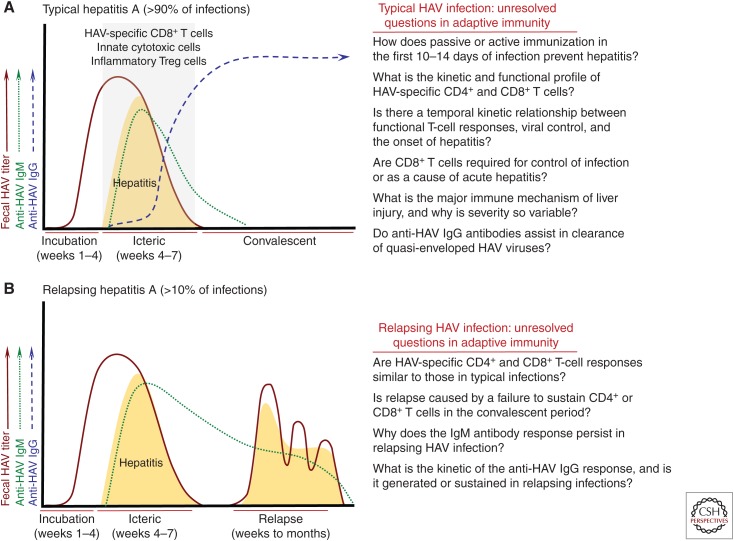
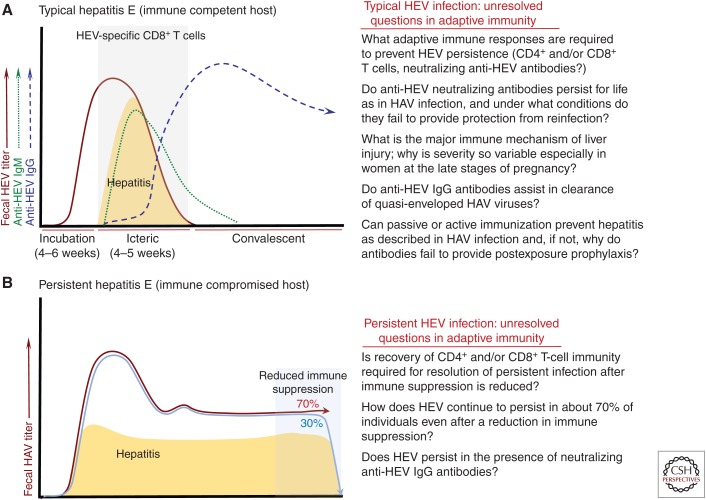
Both hepatitis A virus (HAV) and hepatitis E virus (HEV) cause self-limited infections in humans that are preventable by vaccination. Progress in characterizing adaptive immune responses against these enteric hepatitis viruses, and how they contribute to resolution of infection or liver injury, has therefore remained largely frozen for the past two decades. How HAV and HEV infections are so effectively controlled by B- and T-cell immunity, and why they do not have the same propensity to persist as HBV and HCV infections, cannot yet be adequately explained. The objective of this review is to summarize our understanding of the relationship between patterns of virus replication, adaptive immune responses, and acute liver injury in HAV and HEV infections. Gaps in knowledge, and recent studies that challenge long-held concepts of how antibodies and T cells contribute to control and pathogenesis of HAV and HEV infections, are highlighted.
Copyright © 2019 Cold Spring Harbor Laboratory Press; all rights reserved.
Figures
Similar articles
-
Nonhuman Primate Models of Hepatitis A Virus and Hepatitis E Virus Infections.Cold Spring Harb Perspect Med. 2019 Feb 1;9(2):a031815. doi: 10.1101/cshperspect.a031815. Cold Spring Harb Perspect Med. 2019. PMID: 29686041 Free PMC article. Review.
-
Seroepidemiology of hepatitis A and E virus infections in Tehran, Iran: a population based study.Trans R Soc Trop Med Hyg. 2012 Sep;106(9):528-31. doi: 10.1016/j.trstmh.2012.05.013. Epub 2012 Jul 24. Trans R Soc Trop Med Hyg. 2012. PMID: 22835757
-
Prevalence of hepatitis A, B, C, and E antibody in flying airline personnel.Aviat Space Environ Med. 2000 Dec;71(12):1178-80. Aviat Space Environ Med. 2000. PMID: 11439715
-
A Recombinant HAV Expressing a Neutralization Epitope of HEV Induces Immune Response against HAV and HEV in Mice.Viruses. 2017 Sep 15;9(9):260. doi: 10.3390/v9090260. Viruses. 2017. PMID: 28914805 Free PMC article.
-
Immunity against hepatitis E virus infection: Implications for therapy and vaccine development.Rev Med Virol. 2018 Mar;28(2). doi: 10.1002/rmv.1964. Epub 2017 Dec 22. Rev Med Virol. 2018. PMID: 29272060 Review.
Cited by
-
Cellular and Humoral Immune Profiles After Hepatitis E Vaccination and Infection.Viruses. 2025 Jun 26;17(7):901. doi: 10.3390/v17070901. Viruses. 2025. PMID: 40733519 Free PMC article.
-
Hepatitis A: Epidemiology, Natural History, Unusual Clinical Manifestations, and Prevention.Gastroenterol Clin North Am. 2020 Jun;49(2):191-199. doi: 10.1016/j.gtc.2020.01.002. Epub 2020 Mar 29. Gastroenterol Clin North Am. 2020. PMID: 32389358 Free PMC article. Review.
-
Atomic force microscopy at the forefront: unveiling foodborne viruses with biophysical tools.Npj Viruses. 2025 Apr 4;3(1):25. doi: 10.1038/s44298-025-00107-y. Npj Viruses. 2025. PMID: 40295860 Free PMC article. Review.
-
Seroprevalence of hepatitis A and hepatitis E in patients at a teaching hospital of northern India over a period of 8 years.J Family Med Prim Care. 2022 Feb;11(2):567-572. doi: 10.4103/jfmpc.jfmpc_1212_21. Epub 2022 Feb 16. J Family Med Prim Care. 2022. PMID: 35360807 Free PMC article.
-
Unveiling the Burden of Hepatitis A in Salerno, Italy: A Comprehensive 9-Year Retrospective Study (2015-2023) on the Seroprevalence of HAV Antibodies and Age/Sex Distribution.J Clin Med. 2024 Sep 18;13(18):5534. doi: 10.3390/jcm13185534. J Clin Med. 2024. PMID: 39337021 Free PMC article.
References
-
- Abravanel F, Barrague H, Dorr G, Saune K, Peron JM, Alric L, Kamar N, Izopet J, Champagne E. 2016. Conventional and innate lymphocytes response at the acute phase of HEV infection in transplanted patients. J Infect 72: 723–730. - PubMed
-
- Al-Ayoubi J, Behrendt P, Bremer B, Suneetha PV, Gisa A, Rinker F, Manns MP, Cornberg M, Wedemeyer H, Kraft ARM. 2018. Hepatitis E virus ORF 1 induces proliferative and functional T-cell responses in patients with ongoing and resolved hepatitis E. Liver Int 38: 266–277. - PubMed
-
- Balayan MS, Andjaparidze AG, Savinskaya SS, Ketiladze ES, Braginsky DM, Savinov AP, Poleschuk VF. 1983. Evidence for a virus in non-A, non-B hepatitis transmitted via the fecal–oral route. Intervirology 20: 23–31. - PubMed
-
- Behrendt P, Luth S, Dammermann W, Drave S, Brown RJ, Todt D, Schnoor U, Steinmann E, Wedemeyer H, Pischke S, et al. 2017. Exacerbation of hepatitis E virus infection during anti-TNFα treatment. Joint Bone Spine 84: 217–219. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous