

Less invasive surfactant administration and complications of preterm birth
- PMID: 29844331
- PMCID: PMC5974027
- DOI: 10.1038/s41598-018-26437-x
Less invasive surfactant administration and complications of preterm birth
Abstract
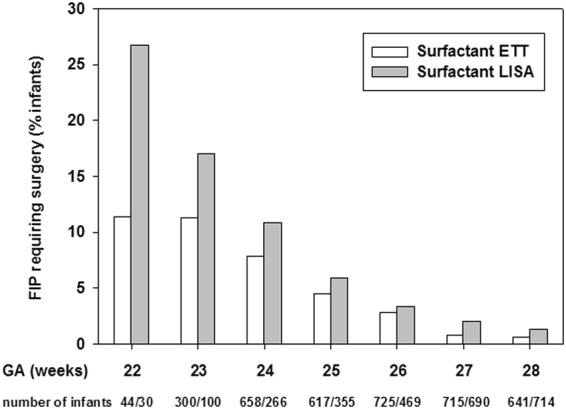
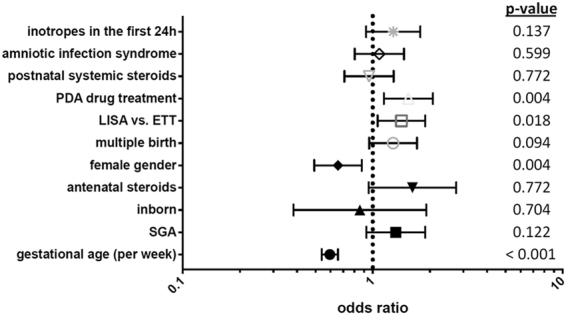
In a large cohort study of the German Neonatal Network (GNN) we aimed to evaluate whether less invasive surfactant administration (LISA) strategy is associated with complications of preterm birth. Within the observational period n = 7533 very-low-birth-weight infants (VLBWI) with gestational age 22 0/7 to 28 6/7 weeks were enrolled in GNN; n = 1214 VLBWI never received surfactant, n = 2624 VLBWI were treated according to LISA procedure, n = 3695 VLBWI had surfactant via endotracheal tube (ETT). LISA was associated with a reduced risk for adverse outcome measures including mortality [odds ratio (OR) 0.66 (95% CI: 0.51-0.84), p < 0.001] bronchopulmonary dysplasia [BPD; OR 0.55 (95% CI: 0.49-0.62), p < 0.001], intracerebral hemorrhage (ICH) grade II-IV [OR 0.55 (95% CI: 0.48-0.64), p < 0.001] and retinopathy of prematurity [ROP; OR 0.62 (95% CI: 0.45-0.85), p < 0.001]. Notably, LISA was associated with an increased risk for focal intestinal perforation [FIP; OR 1.49 (95% CI: 1.14-1.95), p = 0.002]. The differences in FIP rates were primarily observed in VLBWI born <26 weeks (LISA: 10.0 vs. ETT: 7.4%, p = 0.029). Our observational data confirm that LISA is associated with improved outcome. In infants <26 weeks we noted an increased risk for FIP. Future randomized controlled trials including LISA need to integrate safety analyses for this particular subgroup.
Conflict of interest statement
Christoph Härtel, Egbert Herting and Wolfgang Göpel have received funding for a clinical study and have received payments for advisory board duties from Chiesi Pharmaceuticals, Parma, Italy. All other authors have indicated that they have no financial relationships relevant to this article to disclose.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
