

Phase IV study of retention on fingolimod versus injectable multiple sclerosis therapies: a randomized clinical trial
- PMID: 29844796
- PMCID: PMC5964857
- DOI: 10.1177/1756286418774338
Phase IV study of retention on fingolimod versus injectable multiple sclerosis therapies: a randomized clinical trial
Abstract
Objective: In relapsing-remitting multiple sclerosis (RRMS), suboptimal adherence to injectable disease-modifying therapies (iDMTs; interferon β-1a/b, glatiramer acetate) is common, reducing their effectiveness. Patient retention on oral fingolimod and iDMTs was evaluated in PREFERMS, a randomized, parallel-group, active-controlled, open-label, 48-week study.
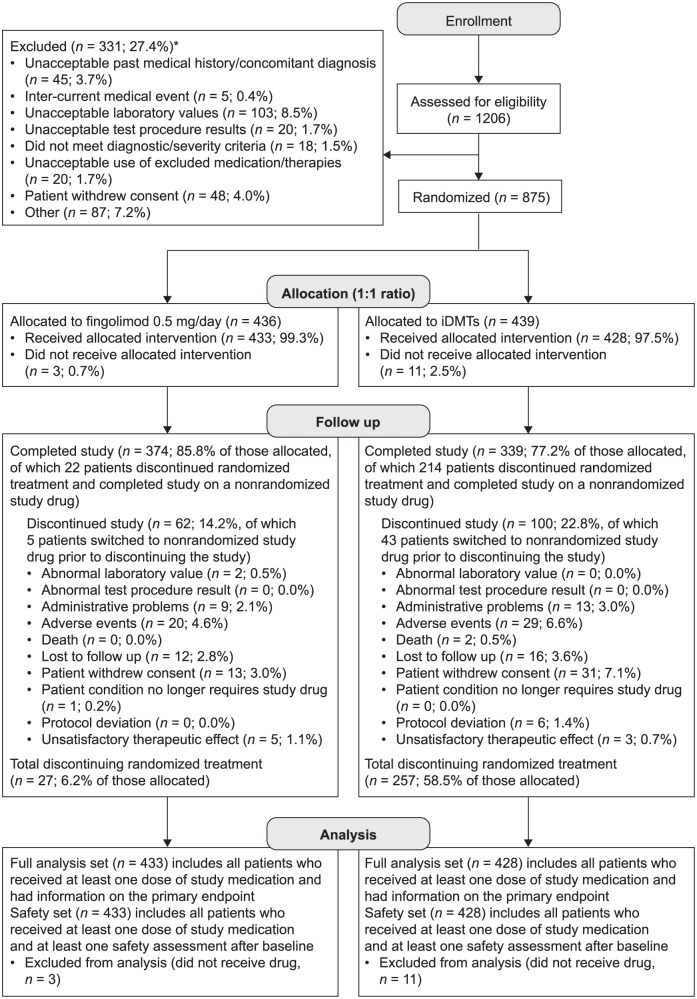
Methods: Patients were included if they had RRMS, were aged 18-65 years and had Expanded Disability Status Scale score up to 6, enrolled at 117 US study sites, were treatment naïve or had received only one iDMT class. Patients were randomized 1:1 (fingolimod 0.5 mg/day; preselected iDMT) by interactive voice-and-web-response system without blinding, followed up quarterly, and allowed one study-approved treatment switch after 12 weeks, or earlier for efficacy or safety reasons. The primary outcome was patient retention on randomized treatment over 48 weeks. Secondary endpoints included patient-reported outcomes, brain volume loss (BVL), and cognitive function.
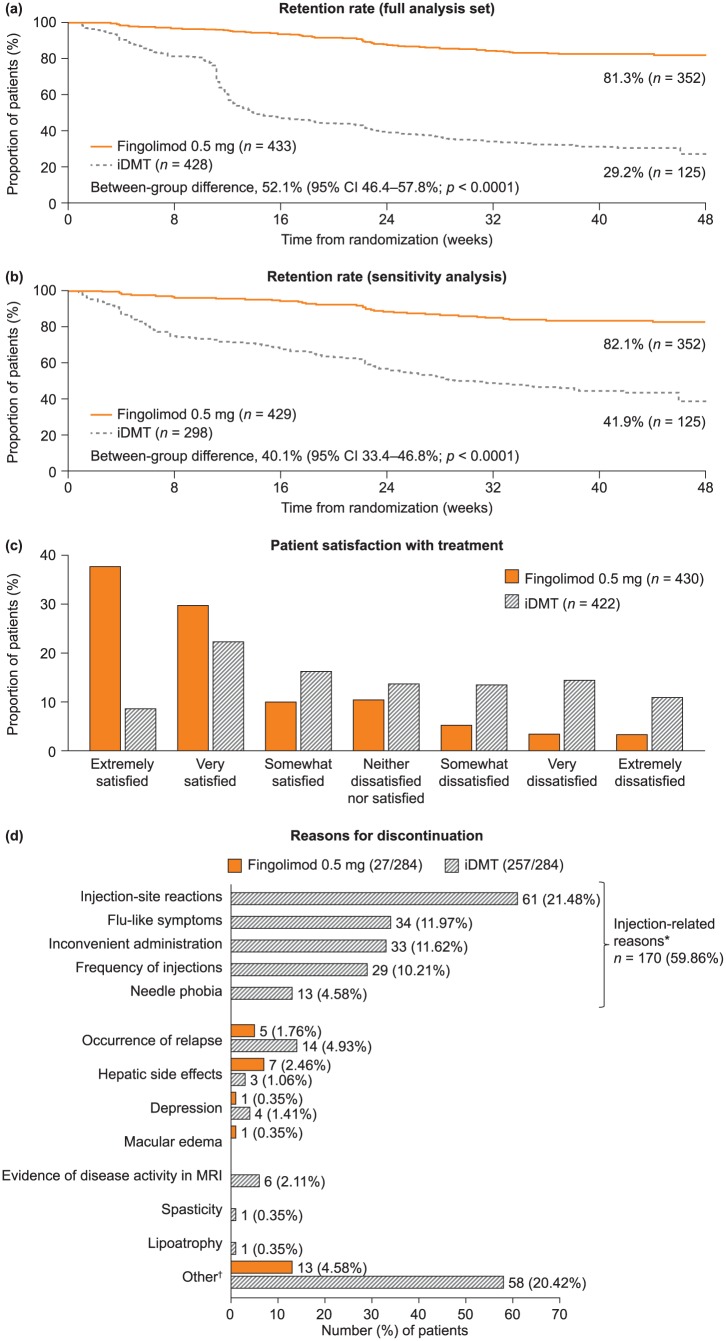
Results: Analysis of 433/436 patients receiving fingolimod and 428/439 receiving iDMTs showed that patient retention rate was significantly higher with fingolimod than with iDMTs [352 (81.3%) versus 125 (29.2%); 95% confidence interval 46.4-57.8%; p < 0.0001]. The most common treatment switch was from iDMT to fingolimod for injection-related reasons. Patient satisfaction was greater and BVL less with fingolimod than with iDMTs, with no difference in cognitive function. Adverse events were consistent with established tolerability profiles for each treatment.
Conclusions: In RRMS, fingolimod was associated with better treatment retention, patient satisfaction and BVL outcomes than iDMTs. Patients may persist with iDMTs, but many may switch treatment if permitted. Treatment satisfaction fosters adherence, a prerequisite for optimal outcomes.
Keywords: adherence; disease-modifying therapy; fingolimod; glatiramer acetate; interferon; multiple sclerosis; randomized controlled trial; retention.
Conflict of interest statement
Conflict of interest statement: BACC has received personal compensation for consulting from AbbVie, Biogen, EMD Serono, GeNEuro, Novartis and Sanofi Genzyme. DLA has an equity interest in NeuroRx Research, and has received personal fees from Acorda Therapeutics, Biogen, EMD Serono, Genentech, Genzyme, Hoffmann-La Roche, MedImmune, Mitsubishi, Novartis, Receptos, and Sanofi-Aventis, and grants from Biogen and Novartis. MC has received research support or consulting fees from Acorda Therapeutics, Bayer HealthCare, Biogen Idec, EMD Serono, Genzyme, Genentech, Novartis, Roche, and Sanofi Aventis. EJF has received consultancy fees, honoraria, and travel or research support from Acorda Therapeutics, Bayer, Biogen, Chugai, Eli Lilly, EMD Serono, Genzyme, Novartis, Ono, Opexa Therapeutics, Roche, Sanofi, and Teva Neuroscience. IMW is an employee of Oxford PharmaGenesis. XM, LS, and NT are employees of Novartis Pharmaceuticals Corporation.
Figures

References
-
- Coyle PK. Switching algorithms: from one immunomodulatory agent to another. J Neurol 2008; 255(Suppl. 1): 44–50. - PubMed
-
- Devonshire V, Lapierre Y, Macdonell R, et al. The Global Adherence Project (GAP): a multicenter observational study on adherence to disease-modifying therapies in patients with relapsing-remitting multiple sclerosis. Eur J Neurol 2011; 18: 69–77. - PubMed
-
- Gajofatto A, Bacchetti P, Grimes B, et al. Switching first-line disease-modifying therapy after failure: impact on the course of relapsing-remitting multiple sclerosis. Mult Scler 2009; 15: 50–58. - PubMed
-
- Scolding N, Barnes D, Cader S, et al. Association of British Neurologists: revised (2015) guidelines for prescribing disease-modifying treatments in multiple sclerosis. Pract Neurol 2015; 15: 273–279. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
