

Clinical implementation of electric impedance tomography in the treatment of ARDS: a single centre experience
- PMID: 29845479
- PMCID: PMC6420412
- DOI: 10.1007/s10877-018-0164-x
Clinical implementation of electric impedance tomography in the treatment of ARDS: a single centre experience
Abstract
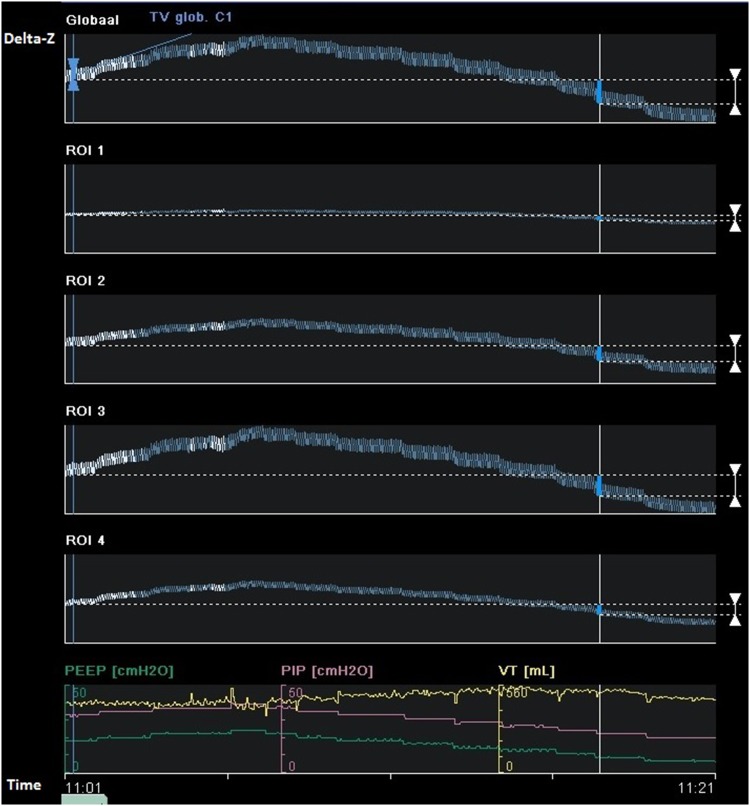
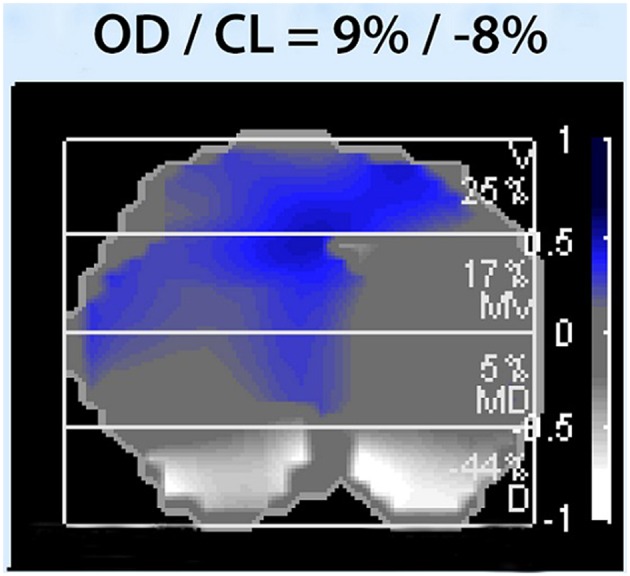
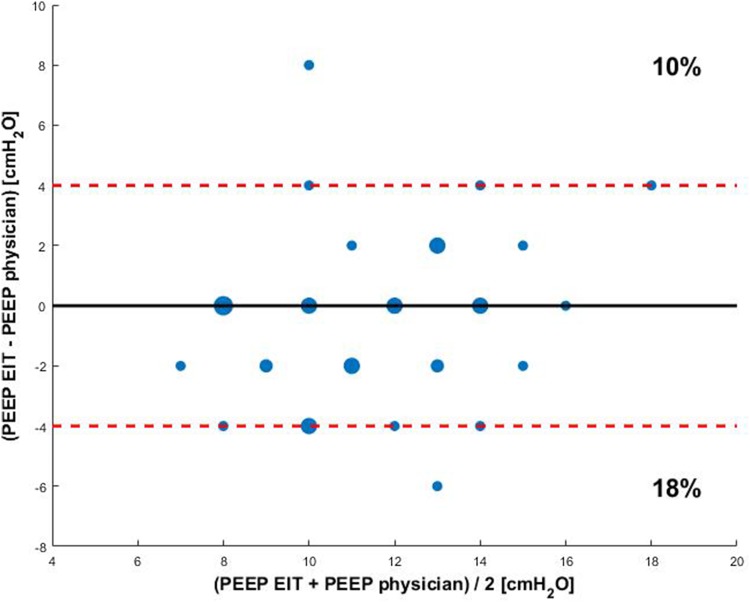
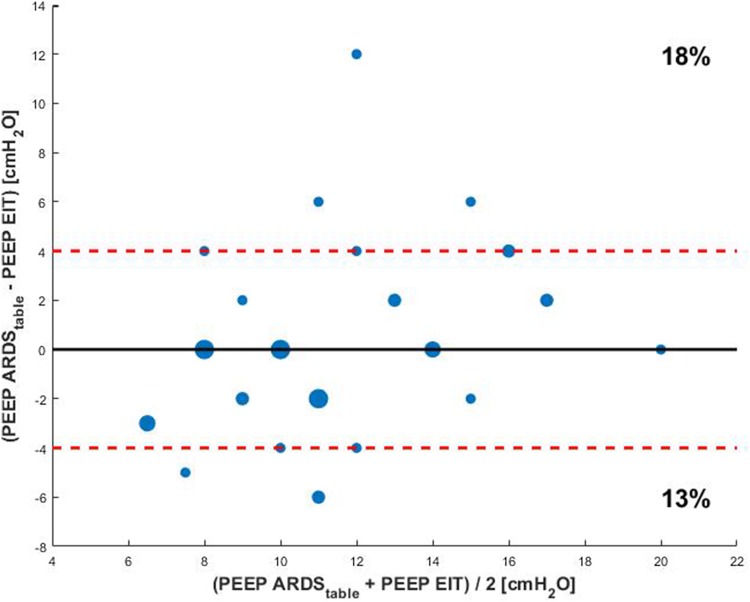
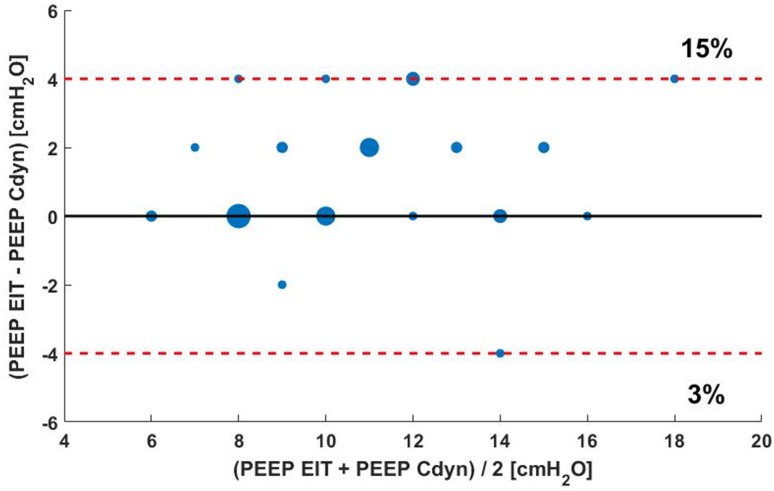
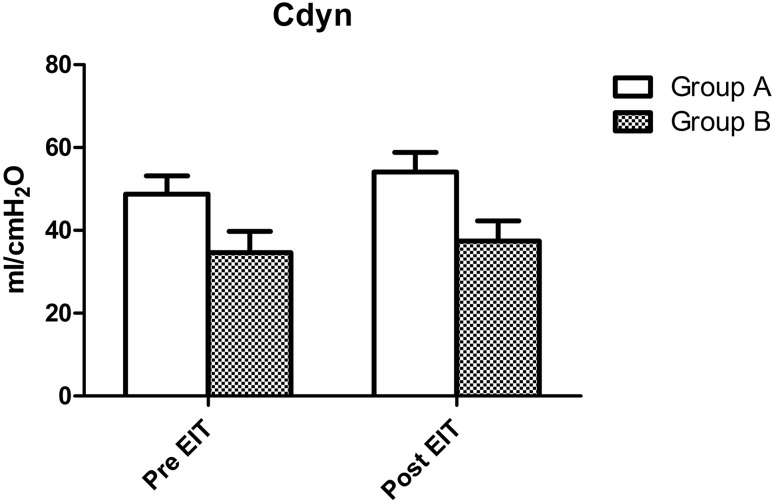
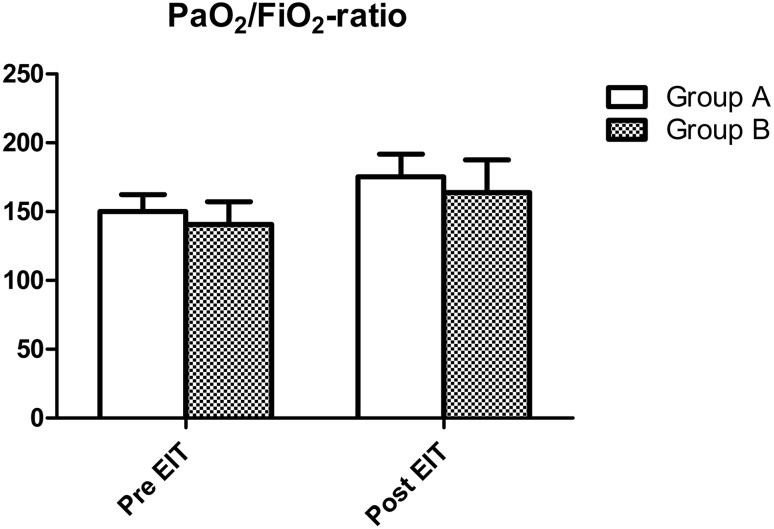
To report on our clinical experience using EIT in individualized PEEP titration in ARDS. Using EIT assessment, we optimized PEEP settings in 39 ARDS patients. The EIT PEEP settings were compared with the physicians' PEEP settings and the PEEP settings according to the ARDS network. We defined a PEEP difference equal to or greater than 4 cm H2O as clinically relevant. Changes in lung compliance and PaO2/FiO2-ratio were compared in patients with EIT-based PEEP adjustments and in patients with unaltered PEEP. In 28% of the patients, the difference in EIT-based PEEP and physician-PEEP was clinically relevant; in 36%, EIT-based PEEP and physician-PEEP were equal. The EIT-based PEEP disagreed with the PEEP settings according to the ARDS network. Adjusting PEEP based upon EIT led to a rapid increase in lung compliance and PaO2/FiO2-ratio. However, this increase was also observed in the group where the PEEP difference was less than 4 cm H2O. We hypothesize that this can be attributed to the alveolar recruitment during the PEEP trial. EIT based individual PEEP setting appears to be a promising method to optimize PEEP in ARDS patients. The clinical impact, however, remains to be established.
Keywords: Acute respiratory distress syndrome; Electrical impedance tomography; Mechanical ventilation; Positive end expiratory pressure.
Figures
References
-
- Kallet RH, Branson RD. Do the NIH ARDS clinical trials network PEEP/FiO2 tables provide the best evidence-based guide to balancing PEEP and FiO2 settings in adults? Respir Care. 2007;52(4):461–475. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
