

Inhibition of Tissue Factor Pathway Inhibitor (TFPI) as a Treatment for Haemophilia: Rationale with Focus on Concizumab
- PMID: 29845491
- PMCID: PMC6013504
- DOI: 10.1007/s40265-018-0922-6
Inhibition of Tissue Factor Pathway Inhibitor (TFPI) as a Treatment for Haemophilia: Rationale with Focus on Concizumab
Erratum in
-
Correction to: Inhibition of Tissue Factor Pathway Inhibitor (TFPI) as a Treatment for Haemophilia: Rationale with Focus on Concizumab.Drugs. 2018 Jun;78(9):891. doi: 10.1007/s40265-018-0933-3. Drugs. 2018. PMID: 29931593 Free PMC article.
Abstract
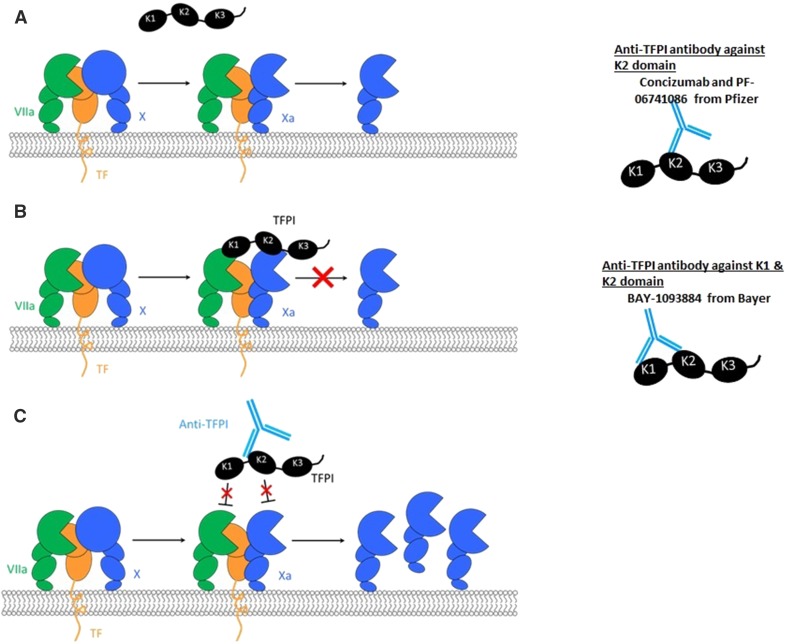
Replacement therapy with missing factor (F) VIII or IX in haemophilia patients for bleed management and preventative treatment or prophylaxis is standard of care. Restoration of thrombin generation through novel mechanisms has become the focus of innovation to overcome limitations imposed by protein replacement therapy. Tissue factor pathway inhibitor (TFPI) is a multivalent Kunitz-type serine protease inhibitor that regulates tissue factor (TF)-induced coagulation through a FXa-dependent feedback inhibition of the TF.FVIIa complex in plasma and on endothelial surfaces. Concizumab is a monoclonal, humanised antibody, specific for the second Kunitz domain of TFPI that binds and inhibits FXa, abolishing the inhibitory effect of TFPI. Concizumab restored thrombin generation in FVIII and FIX deficient plasmas and decreased blood loss in a rabbit haemophilia model. Phase 1 single and multiple dose escalation studies in haemophilia patients demonstrated a dose dependent decrease in TFPI levels and a pro-coagulant effect with increasing d-dimers and prothrombin fragment 1 + 2. A dose dependent increase in peak thrombin and endogenous thrombin potential was observed with values in the normal range when plasma TFPI levels were nearly undetectable. A few haemophilia patients in the highest dose cohorts with complete inhibition of plasma TFPI showed a decreased fibrinogen concentration with normal levels of anti-thrombin and platelets and no evidence of thrombosis. Pharmacokinetic parameters were influenced by binding to the target (TFPI), demonstrating target mediated drug disposition. A trend towards decreasing bleeding tendency was observed and this preventative effect is being studied in Phase 2 studies with additional data gathered to improve our understanding of the therapeutic window and potential for thrombosis.
Conflict of interest statement
Funding
No external funding was used in the preparation of this manuscript.
Conflict of interest
PC reports, grants and personal fees from Pfizer, grants, personal fees and non-financial support from Bayer, personal fees and non-financial support from Baxalta (Shire), grants, personal fees and non-financial support from CSL Behring, grants, personal fees and non-financial support from NovoNordisk, grants, personal fees and non-financial support from Swedish Orphan Biovitrum AB (Sobi), personal fees from Freeline, personal fees from Roche, outside the submitted work.
Figures
References
-
- White GC, 2nd, Rosendaal F, Aledort LM, Lusher JM, Rothschild C, Ingerslev J. Definitions in haemophilia. Recommendation of the scientific subcommittee on factor VIII and factor IX of the scientific and standardization committee of the International Society on Thrombosis and Haemostasis. Thromb Haemost. 2001;85(3):560. doi: 10.1055/s-0037-1615621. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
