

Sinonasal Ameloblastoma
- PMID: 29846904
- PMCID: PMC6514030
- DOI: 10.1007/s12105-018-0933-3
Sinonasal Ameloblastoma
Abstract
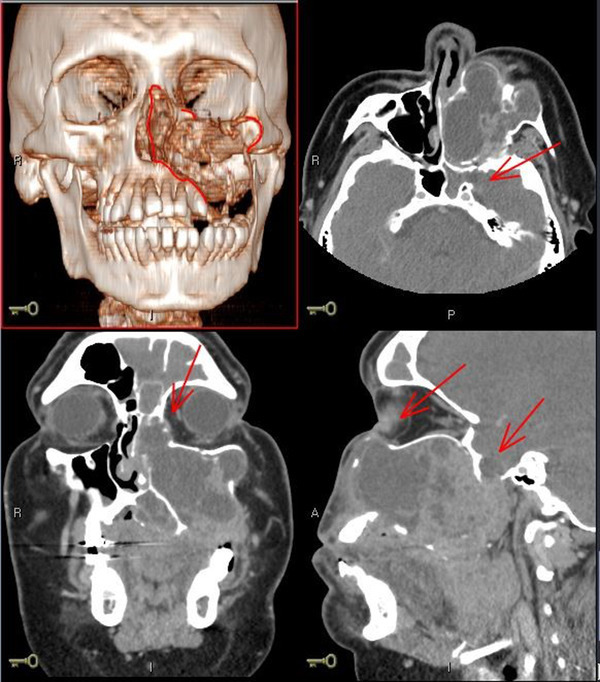
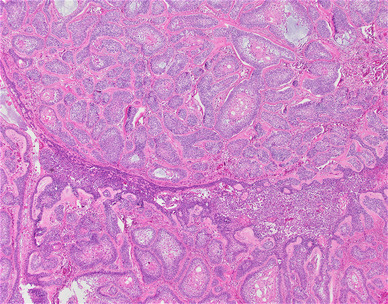
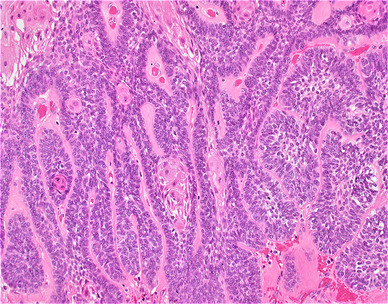
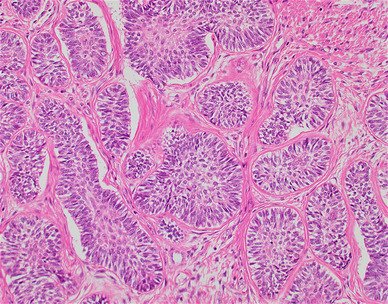
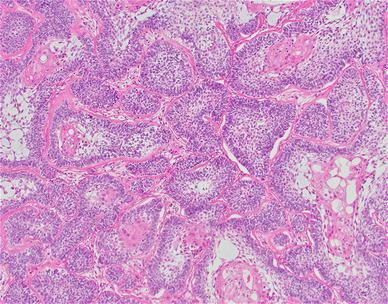
Ameloblastomas are benign but aggressive odontogenic tumors that most commonly affect the posterior mandible. Approximately 15% occur in the maxilla, with a subset thought to originate from the epithelial lining of the sinonasal cavities. Histologically, sinonasal ameloblastomas are identical to those of the oral cavity, with classical features of palisaded columnar basilar cells surrounding a central proliferation that resembles the stellate reticulum of a developing tooth. Unlike the gnathic variant, sinonasal ameloblastomas tend to affect males more than females, and the incidence of diagnosis peaks at a later age, approximately 60 years old. The overall prognosis is favorable, with local recurrence being the most common long-term sequalae.
Keywords: Gnathic; Maxilla; Odontogenic neoplasm; Sinonasal ameloblastoma.
Figures
References
-
- El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ. WHO classification of head and neck tumours. 4. IARC: Lyon; 2017.
-
- Kumar A, Sarswat S, Sharma S. Ameloblastoma presenting as a sinonasal tumor: rare entity. Int J Adv Health Sci. 2014;1(2):28–31.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
