

The impact of the rising colorectal cancer incidence in young adults on the optimal age to start screening: Microsimulation analysis I to inform the American Cancer Society colorectal cancer screening guideline
- PMID: 29846933
- PMCID: PMC6033623
- DOI: 10.1002/cncr.31543
The impact of the rising colorectal cancer incidence in young adults on the optimal age to start screening: Microsimulation analysis I to inform the American Cancer Society colorectal cancer screening guideline
Abstract
Background: In 2016, the Microsimulation Screening Analysis-Colon (MISCAN-Colon) model was used to inform the US Preventive Services Task Force colorectal cancer (CRC) screening guidelines. In this study, 1 of 2 microsimulation analyses to inform the update of the American Cancer Society CRC screening guideline, the authors re-evaluated the optimal screening strategies in light of the increase in CRC diagnosed in young adults.
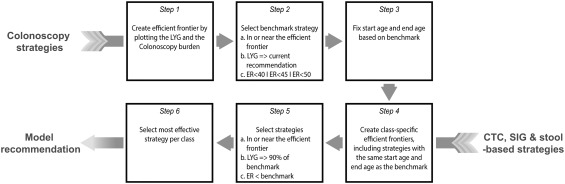
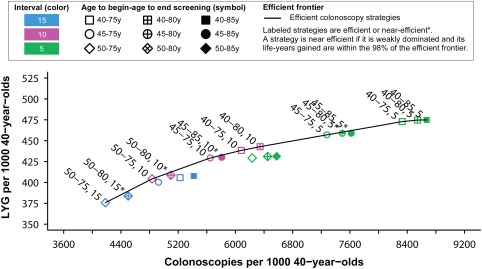
Methods: The authors adjusted the MISCAN-Colon model to reflect the higher CRC incidence in young adults, who were assumed to carry forward escalated disease risk as they age. Life-years gained (LYG; benefit), the number of colonoscopies (COL; burden) and the ratios of incremental burden to benefit (efficiency ratio [ER] = ΔCOL/ΔLYG) were projected for different screening strategies. Strategies differed with respect to test modality, ages to start (40 years, 45 years, and 50 years) and ages to stop (75 years, 80 years, and 85 years) screening, and screening intervals (depending on screening modality). The authors then determined the model-recommended strategies in a similar way as was done for the US Preventive Services Task Force, using ER thresholds in accordance with the previously accepted ER of 39.
Results: Because of the higher CRC incidence, model-predicted LYG from screening increased compared with the previous analyses. Consequently, the balance of burden to benefit of screening improved and now 10-yearly colonoscopy screening starting at age 45 years resulted in an ER of 32. Other recommended strategies included fecal immunochemical testing annually, flexible sigmoidoscopy screening every 5 years, and computed tomographic colonography every 5 years.
Conclusions: This decision-analysis suggests that in light of the increase in CRC incidence among young adults, screening may be offered earlier than has previously been recommended. Cancer 2018;124:2964-73. © 2018 The Authors. Cancer published by Wiley Periodicals, Inc. on behalf of American Cancer Society.
Keywords: advisory committees; colorectal neoplasms; early detection of cancer; incidence; models; preventive health services; theoretical.
© 2018 The Authors. Cancer published by Wiley Periodicals, Inc. on behalf of American Cancer Society.
Figures
References
-
- American Cancer Society . Cancer statistics center. https://cancerstatisticscenter.cancer.org/?_ga=1.33682849.1877282425.146.... Accessed April 30, 2018.
-
- Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67:177‐193. - PubMed
-
- Bibbins‐Domingo K, Grossman DC, Curry SJ, et al. Screening for colorectal cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2016;315:2564‐2575. - PubMed
-
- Levin B, Lieberman DA, McFarland B, et al; American Cancer Society Colorectal Cancer Advisory Group; US Multi‐Society Task Force; American College of Radiology Colon Cancer Committee . Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi‐Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58:130‐160. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
