

Optimizing colorectal cancer screening by race and sex: Microsimulation analysis II to inform the American Cancer Society colorectal cancer screening guideline
- PMID: 29846942
- PMCID: PMC6055229
- DOI: 10.1002/cncr.31542
Optimizing colorectal cancer screening by race and sex: Microsimulation analysis II to inform the American Cancer Society colorectal cancer screening guideline
Abstract
Background: Colorectal cancer (CRC) risk varies by race and sex. This study, 1 of 2 microsimulation analyses to inform the 2018 American Cancer Society CRC screening guideline, explored the influence of race and sex on optimal CRC screening strategies.
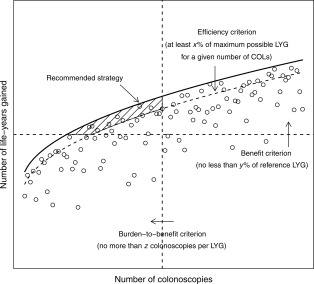
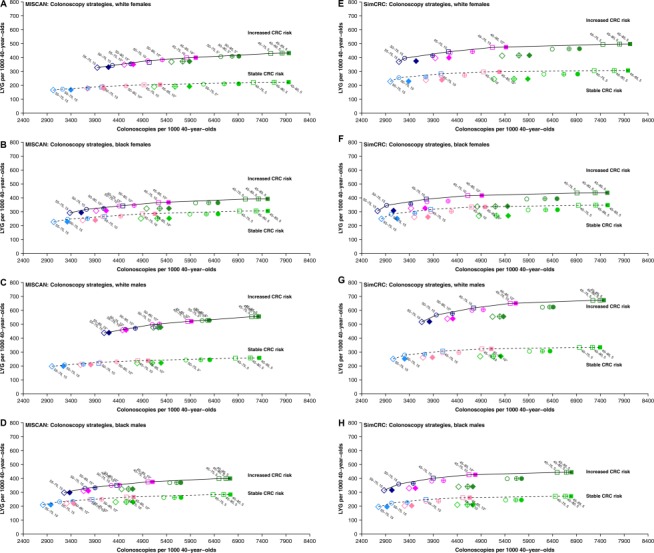
Methods: Two Cancer Intervention and Surveillance Modeling Network microsimulation models, informed by US incidence data, were used to evaluate a variety of screening methods, ages to start and stop, and intervals for 4 demographic subgroups (black and white males and females) under 2 scenarios for the projected lifetime CRC risk for 40-year-olds: 1) assuming that risk had remained stable since the early screening era and 2) assuming that risk had increased proportionally to observed incidence trends under the age of 40 years. Model-based screening recommendations were based on the predicted level of benefit (life-years gained) and burden (required number of colonoscopies), the incremental burden-to-benefit ratio, and the relative efficiency in comparison with strategies with similar burdens.
Results: When lifetime CRC risk was assumed to be stable over time, the models differed in the recommended age to start screening for whites (45 vs 50 years) but consistently recommended screening from the age of 45 years for blacks. When CRC risk was assumed to be increased, the models recommended starting at the age of 45 years, regardless of race and sex. Strategies recommended under both scenarios included colonoscopy every 10 or 15 years, annual fecal immunochemical testing, and computed tomographic colonography every 5 years through the age of 75 years.
Conclusions: Microsimulation modeling suggests that CRC screening should be considered from the age of 45 years for blacks and for whites if the lifetime risk has increased proportionally to the incidence for younger adults. Cancer 2018;124:2974-85. © 2018 The Authors. Cancer published by Wiley Periodicals, Inc. on behalf of American Cancer Society.
Keywords: colorectal neoplasms; decision modeling; early detection of cancer; guidelines; personalized medicine.
© 2018 The Authors. Cancer published by Wiley Periodicals, Inc. on behalf of American Cancer Society.
Figures
References
-
- Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin. 2017;67:177‐193. - PubMed
-
- Winawer SJ, Fletcher RH, Miller L, et al. Colorectal cancer screening: clinical guidelines and rationale. Gastroenterology. 1997;112:594‐642. - PubMed
-
- Eddy D. ACS report on the cancer‐related health checkup. CA Cancer J Clin. 1980;30:193‐240. - PubMed
-
- Arias E, Heron M, Jiaquan X. United States life tables, 2013. Natl Vital Stat Rep. 2017;66:1‐64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
