

Comparison of Efficacy and Safety of 4 Combinations of Laparoscopic and Intraoperative Techniques for Management of Gallstone Disease With Biliary Duct Calculi: A Systematic Review and Network Meta-analysis
- PMID: 29847616
- PMCID: PMC6137518
- DOI: 10.1001/jamasurg.2018.1167
Comparison of Efficacy and Safety of 4 Combinations of Laparoscopic and Intraoperative Techniques for Management of Gallstone Disease With Biliary Duct Calculi: A Systematic Review and Network Meta-analysis
Abstract
Importance: Several techniques are used for surgical treatment of gallstone disease with biliary duct calculi, but the safety and efficacy of these approaches have not been compared.
Objectives: To compare the efficacy and safety of 4 surgical approaches to gallstone disease with biliary duct calculi.
Data sources: MEDLINE, Scopus, and ISI-Web of Science databases, articles published between 1950 and 2017 and searched from August 12, 2017, to September 14, 2017. Search terms used were LCBDE, LC, preoperative, ERCP, postoperative, period, cholangiopancreatography, endoscopic, retrograde, rendezvous, intraoperative, one-stage, two-stage, single-stage, gallstone, gallstones, calculi, stone, therapy, treatment, therapeutics, surgery, surgical, procedures, clinical trials as topic, random, and allocation in several logical combinations.
Study selection: Randomized clinical trials comparing at least 2 of the following strategies: preoperative endoscopic retrograde cholangiopancreatography (PreERCP) plus laparoscopic cholecystectomy (LC); LC with laparoscopic common bile duct exploration (LCDBE); LC plus intraoperative endoscopic retrograde cholangiopancreatography (IntraERCP); and LC plus postoperative ERCP (PostERCP).
Data extraction and synthesis: A frequentist random-effects network meta-analysis was performed. The surface under the cumulative ranking curve (SUCRA) was used to show the probability that each approach would be the best for each outcome.
Main outcomes and measures: Primary outcomes were the safety to efficacy ratio using overall mortality and morbidity rates as the main indicators of safety and the success rate as an indicator of efficacy. Secondary outcomes were acute pancreatitis, biliary leak, overall bleeding, operative time, length of hospital stay, total cost, and readmission rate.
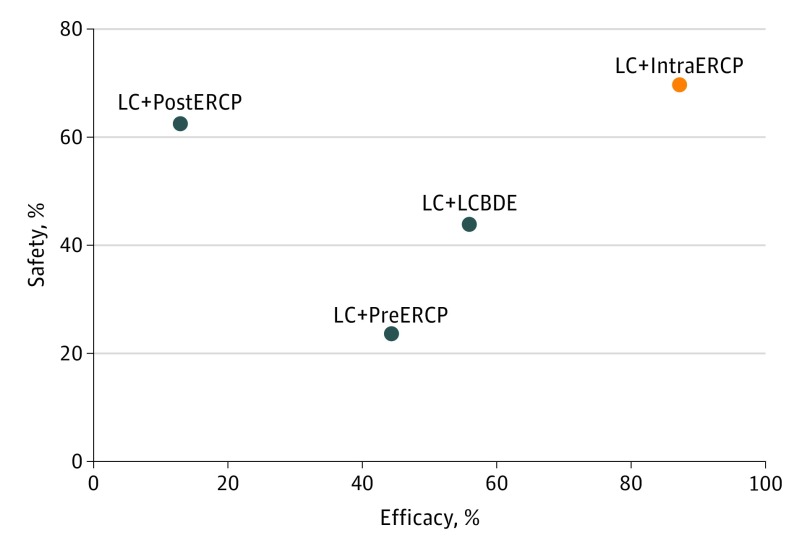
Results: The 20 trials comprised 2489 patients (and 2489 procedures). Laparoscopic cholecystectomy plus IntraERCP had the highest probability of being the most successful (SUCRA, 87.2%) and safest (SUCRA, 69.7%) with respect to morbidity. All approaches had similar results regarding overall mortality. Laparoscopic cholecystectomy plus LCBDE was the most successful for avoiding overall bleeding (SUCRA, 83.3%) and for the shortest operative time (SUCRA, 90.2%) and least total cost (SUCRA, 98.9%). Laparoscopic cholecystectomy plus IntraERCP was the best approach for length of hospital stay (SUCRA, 92.7%). Inconsistency was found in operative time (indirect estimate, 19.05; 95% CI, 2.44-35.66; P = .02) and total cost (indirect estimate, 17.06; 95% CI, 3.56-107.21; P = .04). Heterogeneity was observed for success rate (τ, 0.8), operative time (τ, >1), length of stay (τ, >1), and total cost (τ, >1).
Conclusions and relevance: The combined LC and IntraERCP approach had the greatest odds to be the safest and appears to be the most successful. Laparoscopic cholecystectomy plus LBCDE appears to reduce the risk of acute pancreatitis but may be associated with a higher risk of biliary leak.
Conflict of interest statement
Figures
References
-
- Petelin JB. Laparoscopic common bile duct exploration. Surg Endosc. 2003;17(11):1705-1715. - PubMed
-
- Purkayastha S, Tilney HS, Georgiou P, Athanasiou T, Tekkis PP, Darzi AW. Laparoscopic cholecystectomy versus mini-laparotomy cholecystectomy: a meta-analysis of randomised control trials. Surg Endosc. 2007;21(8):1294-1300. - PubMed
-
- Williams E, Beckingham I, El Sayed G, et al. . Updated guideline on the management of common bile duct stones (CBDS). Gut. 2017;66(5):765-782. - PubMed
-
- Cipriani A, Higgins JP, Geddes JR, Salanti G. Conceptual and technical challenges in network meta-analysis. Ann Intern Med. 2013;159(2):130-137. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
