

Inflammasomes: a novel therapeutic target in pulmonary hypertension?
- PMID: 29847700
- PMCID: PMC6534811
- DOI: 10.1111/bph.14375
Inflammasomes: a novel therapeutic target in pulmonary hypertension?
Abstract
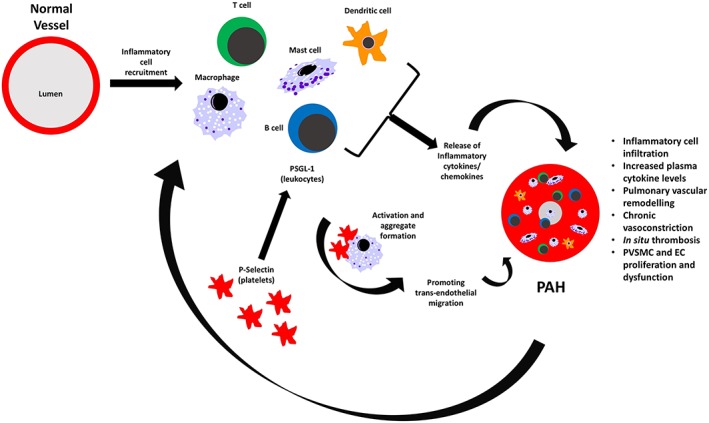
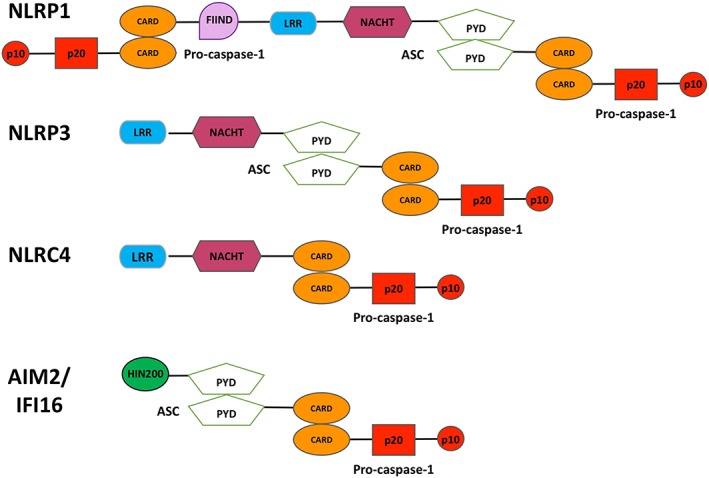
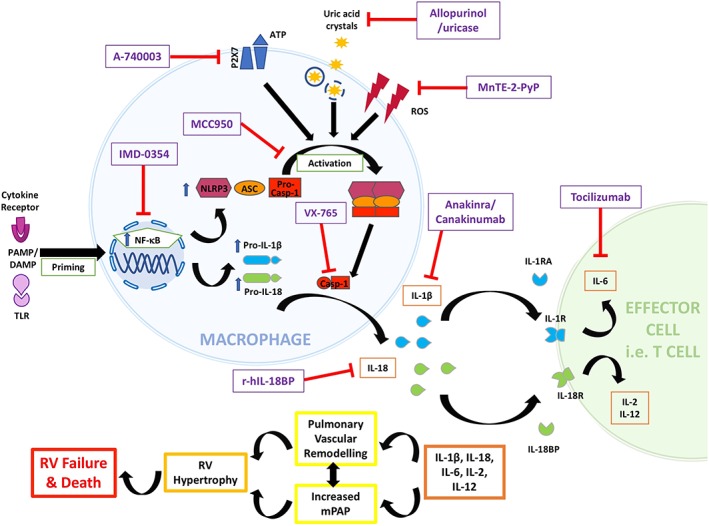
Pulmonary hypertension (PH) is a rare, progressive pulmonary vasculopathy characterized by increased mean pulmonary arterial pressure, pulmonary vascular remodelling and right ventricular failure. Current treatments are not curative, and new therapeutic strategies are urgently required. Clinical and preclinical evidence has established that inflammation plays a key role in PH pathogenesis, and recently, inflammasomes have been suggested to be central to this process. Inflammasomes are important regulators of inflammation, releasing the pro-inflammatory cytokines IL-1β and IL-18 in response to exogenous pathogen- and endogenous damage-associated molecular patterns. These cytokines are elevated in PH patients, but whether this is a consequence of inflammasome activation remains to be determined. This review will briefly summarize current PH therapies and their pitfalls, introduce inflammasomes and the mechanisms by which they promote inflammation and, finally, highlight the preclinical and clinical evidence for the potential involvement of inflammasomes in PH pathobiology and how they may be targeted therapeutically. LINKED ARTICLES: This article is part of a themed section on Immune Targets in Hypertension. To view the other articles in this section visit http://onlinelibrary.wiley.com/doi/10.1111/bph.v176.12/issuetoc.
© 2018 The British Pharmacological Society.
Conflict of interest statement
A.H. has been a consultant/advisory board member for Bayer AG, Serodus ASA and Palatin Technologies Inc.
Figures

References
-
- Abman SH, Hansmann G, Archer SL, Ivy DD, Adatia I, Chung WK et al (2015). Pediatric pulmonary hypertension: guidelines from the American Heart Association and American Thoracic Society. Circulation 132: 2037–2099. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
