

Comparison of procalcitonin, C-reactive protein, white blood cell count and clinical status in diagnosing pneumonia in patients hospitalized with acute exacerbations of COPD: A prospective observational study
- PMID: 29848051
- PMCID: PMC6302976
- DOI: 10.1177/1479972318769762
Comparison of procalcitonin, C-reactive protein, white blood cell count and clinical status in diagnosing pneumonia in patients hospitalized with acute exacerbations of COPD: A prospective observational study
Abstract
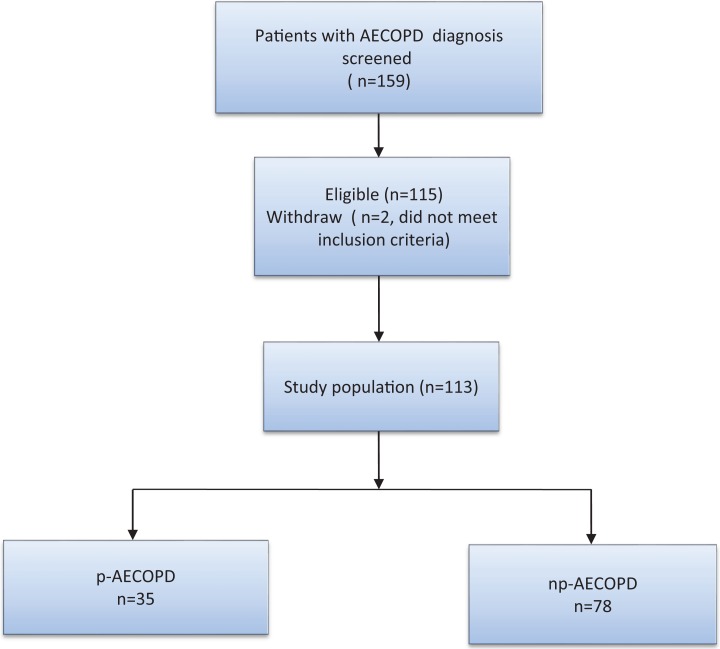
Lower respiratory tract infection is the most common cause of acute exacerbations of chronic obstructive pulmonary disease (AECOPD). The aim of the present study was to compare the accuracy of procalcitonin (PCT), C-reactive protein (CRP) and white blood cell count (WBC) as single diagnostic tests and in combination with clinical signs and symptoms to diagnose pneumonia in patients hospitalized with AECOPD. This was a prospective, single centre observational study. Patients with spirometry-confirmed COPD who were hospitalized due to AECOPD were consecutively recruited at the hospital's Emergency Unit. Pneumonia was defined as a new pulmonary infiltrate on chest X-ray. The values of PCT, CRP and WBC were determined at admission. Receiver operating characteristic (ROC) curve analysis was used to study the accuracy of various diagnostic tests. Of the 113 included patients, 35 (31%) had pneumonia at admission. Area under the ROC curve (AUC) for PCT, CRP and WBC as a single test to distinguish between patients with and without pneumonia was 0.67 (95% CI 0.55-0.79), 0.73 (95% CI 0.63-0.84) and 0.67 (95% CI 0.55-0.79), respectively ( p = 0.42 for the test of difference). The AUC for a model of clinical signs and symptoms was 0.84 (95% CI 0.76-0.92). When biomarkers were added to the clinical model, the AUCs of the combined models were not significantly different from that of the clinical model alone ( p = 0.54). PCT had about the same accuracy as CRP and WBC in predicting pneumonia in patients hospitalized with AECOPD both as a single test and in combination with clinical signs and symptoms.
Keywords: Biomarkers; COPD exacerbation; diagnostic accuracy; pneumonia; serum procalcitonin.
Conflict of interest statement
Figures


Similar articles
-
Neutrophil CD64 Expression as a Diagnostic Marker in Patients Hospitalized with Exacerbations of COPD: A Prospective Observational Study.Lung. 2015 Oct;193(5):717-24. doi: 10.1007/s00408-015-9762-2. Epub 2015 Jul 15. Lung. 2015. PMID: 26174093
-
Comparison of diagnostic values of procalcitonin, C-reactive protein and blood neutrophil/lymphocyte ratio levels in predicting bacterial infection in hospitalized patients with acute exacerbations of COPD.Wien Klin Wochenschr. 2015 Oct;127(19-20):756-63. doi: 10.1007/s00508-014-0690-6. Epub 2015 Jan 14. Wien Klin Wochenschr. 2015. PMID: 25586444
-
Optimal cut-off value of serum procalcitonin in predicting bacterial infection induced acute exacerbation in chronic obstructive pulmonary disease: A prospective observational study.Chron Respir Dis. 2022 Jan-Dec;19:14799731221108516. doi: 10.1177/14799731221108516. Chron Respir Dis. 2022. PMID: 35830291 Free PMC article.
-
Potential of serum procalcitonin in predicting bacterial exacerbation and guiding antibiotic administration in severe COPD exacerbations: a systematic review and meta-analysis.Infect Dis (Lond). 2019 Sep;51(9):639-650. doi: 10.1080/23744235.2019.1644456. Epub 2019 Jul 29. Infect Dis (Lond). 2019. PMID: 31355690
-
Accuracy of Biomarkers for the Diagnosis of Adult Community-acquired Pneumonia: A Meta-analysis.Acad Emerg Med. 2020 Mar;27(3):195-206. doi: 10.1111/acem.13889. Epub 2020 Feb 26. Acad Emerg Med. 2020. PMID: 32100377
Cited by
-
Clinical Significance of Procalcitonin, C-Reactive Protein, and Interleukin-6 in Helping Guide the Antibiotic Use for Patients with Acute Exacerbations of Chronic Obstructive Pulmonary Disease.Dis Markers. 2021 Mar 15;2021:8879401. doi: 10.1155/2021/8879401. eCollection 2021. Dis Markers. 2021. PMID: 33791046 Free PMC article.
-
Sphingosine-1-phosphate and CRP as potential combination biomarkers in discrimination of COPD with community-acquired pneumonia and acute exacerbation of COPD.Respir Res. 2022 Mar 20;23(1):63. doi: 10.1186/s12931-022-01991-1. Respir Res. 2022. PMID: 35307030 Free PMC article.
-
Comparison of CRP, Procalcitonin, Neutrophil Counts, Eosinophil Counts, sTREM-1, and OPN between Pneumonic and Nonpneumonic Exacerbations in COPD Patients.Can Respir J. 2022 Mar 31;2022:7609083. doi: 10.1155/2022/7609083. eCollection 2022. Can Respir J. 2022. PMID: 35400078 Free PMC article.
-
Eosinopenia Predicting Long-term Mortality in Hospitalized Acute Exacerbation of COPD Patients with Community-acquired Pneumonia-A Retrospective Analysis.Int J Chron Obstruct Pulmon Dis. 2021 Dec 30;16:3551-3559. doi: 10.2147/COPD.S347948. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 35002227 Free PMC article.
-
Diagnostic Accuracy of Liquid Biomarkers in Airway Diseases: Toward Point-of-Care Applications.Front Med (Lausanne). 2022 Jun 6;9:855250. doi: 10.3389/fmed.2022.855250. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35733871 Free PMC article. Review.
References
-
- Mullerova H, Maselli DJ, Locantore N, et al. Hospitalized exacerbations of COPD: risk factors and outcomes in the ECLIPSE cohort. Chest 2015; 147: 999–1007. DOI: 10.1378/chest.14-0655. - PubMed
-
- Cilli A. Community-acquired pneumonia in patients with chronic obstructive pulmonary disease. Curr Infect Dis Rep 2015; 17: 444 DOI: 10.1007/s11908-014-0444-7. - PubMed
-
- Mullerova H, Chigbo C, Hagan GW, et al. The natural history of community-acquired pneumonia in COPD patients: a population database analysis. Respir Med 2012; 106: 1124–1133. DOI: 10.1016/j.rmed.2012.04.008. - PubMed
-
- Pifarre R, Falguera M, Vicente-de-Vera C, et al. Characteristics of community-acquired pneumonia in patients with chronic obstructive pulmonary disease. Respir Med 2007; 101: 2139–2144. DOI: 10.1016/j.rmed.2007.05.011. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
