

Review
doi: 10.1177/1591019918777233.
Epub 2018 May 31.
Dural arteriovenous fistula in the sphenoid bone lesser wing region: Endovascular adjuvant techniques of treatment and literature review
Affiliations
- PMID: 29848145
- PMCID: PMC6116136
- DOI: 10.1177/1591019918777233
Item in Clipboard
Review
Dural arteriovenous fistula in the sphenoid bone lesser wing region: Endovascular adjuvant techniques of treatment and literature review
Interv Neuroradiol.
2018 Oct.
Abstract
This article describes the successful endovascular treatment of a dural arteriovenous fistula of a rare localization (the area of sphenoid bone lesser region). We examine one report of an unusually located dural arteriovenous fistula successfully treated with Onyx (ev3, Irvine, USA) using a combination of endovascular adjuvant techniques: pressure cooker and remodeling balloon protection of cerebral artery. The article includes previously published observations of such fistulas and discusses anatomic features and venous drainage of dural arteriovenous fistulas in the given location.
Keywords: Arteriovenous malformation; Onyx; endovascular treatment; technical aspects.
Figures
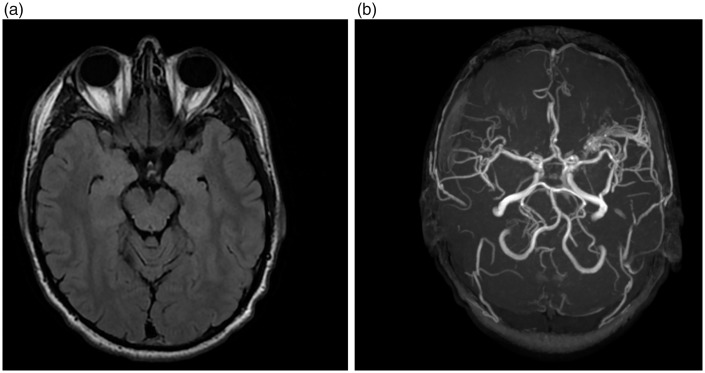
Magnetic resonance imaging (MRI) data. (a) Lack of significant changes in
the left side lesser wing of sphenoid bone at T1- and T2-weighted MRI.
(b) Non-enhanced magnetic resonance angiography (3D-TOF) reveals a dural
arteriovenous fistula.
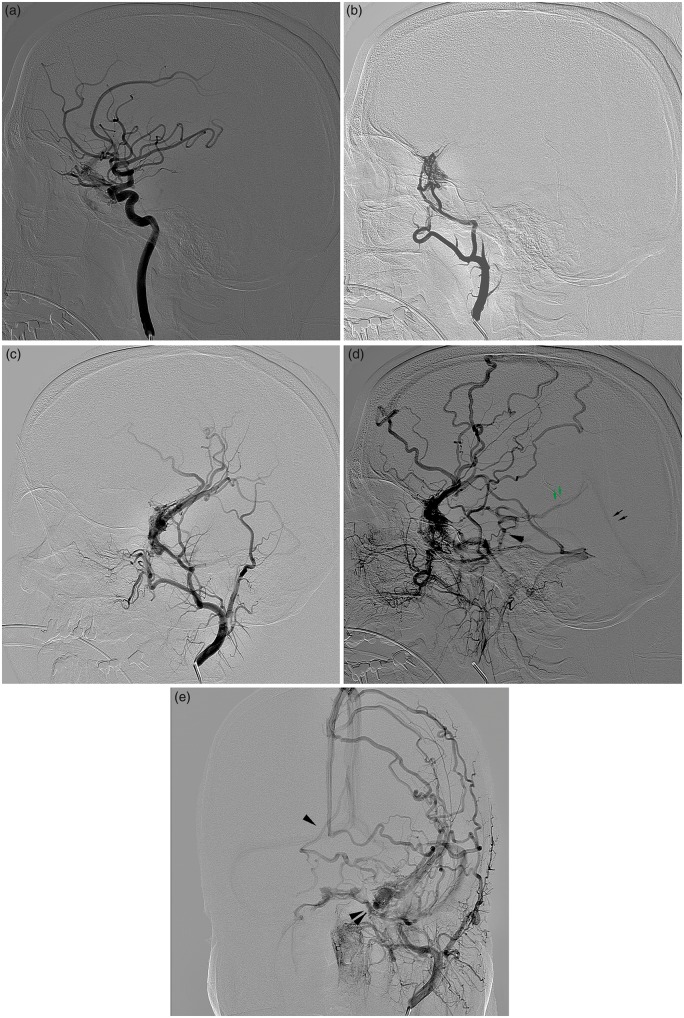
Dural arteriovenous fistula (DAVF) of the lesser sphenoid wing. (a) Dural
arteriovenous shunts fed by recurrent meningeal branch from the
ophthalmic artery and branches from the inferolateral trunk of the
internal carotid artery. (b) DAVF fed by branches arising from the left
middle meningeal artery. Drainage into the superficial cortical veins
with varix. (c) DAVF fed by branches arising from the left middle
meningeal artery. Drainage into the superficial cortical veins with
varix. (d) Venous drainage through superficial cerebral veins into SSS,
paracavernous and superior petrosal sinuses. Retrograde filling into
deep cerebral veins with reflux into the basal vein of Rosenthal via
mesencephalic and peduncular veins, absence of the left of Rosenthal.
(e) Venous drainage through superficial cerebral veins into SSS,
paracavernous and superior petrosal sinuses. Retrograde filling into
deep cerebral veins with reflux into the right basal vein of Rosenthal
via mesencephalic and peduncular veins into the right vein of Rosenthal,
absence of the left vein of Rosenthal.
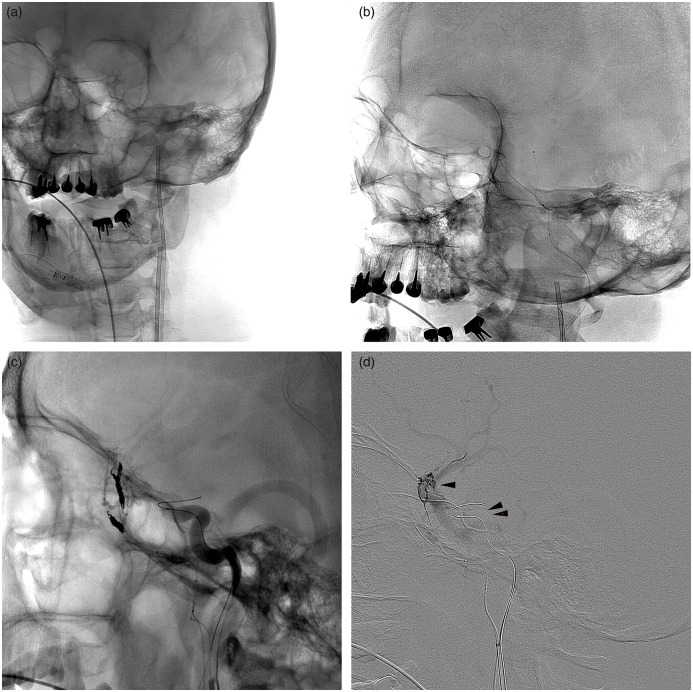
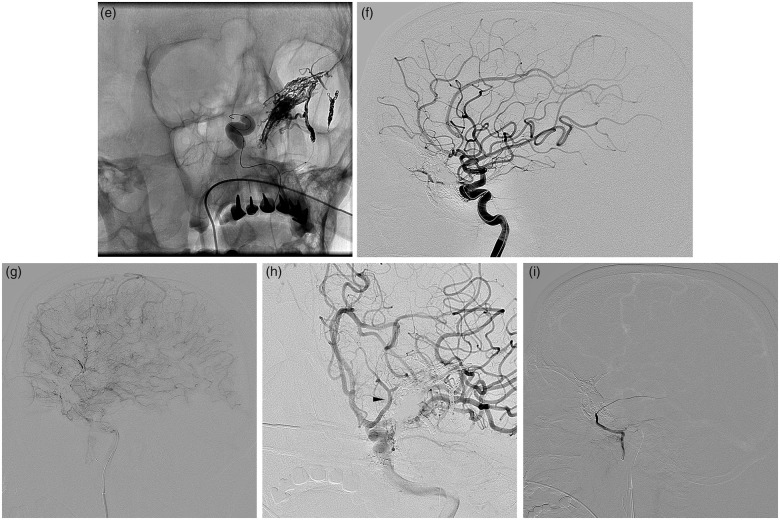
Introduction of microcatheter Apollo 1.5F-5.0 into the frontal branch of
the middle meningeal artery and Excelsior SL-10 microcatheter into the
parietal branch. (a) Placing of two guider catheters into the external
carotid artery (ECA) and internal carotid artery (ICA). (b and c)
Embolization of frontal branches of the middle meningeal artery distally
from the detachment point of the Apollo microcatheter. (d)
Superselective angiography. The superficial middle cerebral vein is
enhanced. (e) Embolization of the fistula with non-adhesive liquid
embolic agent Onyx 18 in a temporary balloon occlusion of the ICA, which
was temporarily inflated at the level of the cavernous segment and
ophthalmic artery origin to eliminate concurrent blood flow and avoid
inadvertent reflux of Onyx into the ICA. (f, g, h) A radical occlusion
of DAVF, preserving the patency of the ophthalmic artery. (i) No filling
of DAVF from the ECA.
Introduction of microcatheter Apollo 1.5F-5.0 into the frontal branch of
the middle meningeal artery and Excelsior SL-10 microcatheter into the
parietal branch. (a) Placing of two guider catheters into the external
carotid artery (ECA) and internal carotid artery (ICA). (b and c)
Embolization of frontal branches of the middle meningeal artery distally
from the detachment point of the Apollo microcatheter. (d)
Superselective angiography. The superficial middle cerebral vein is
enhanced. (e) Embolization of the fistula with non-adhesive liquid
embolic agent Onyx 18 in a temporary balloon occlusion of the ICA, which
was temporarily inflated at the level of the cavernous segment and
ophthalmic artery origin to eliminate concurrent blood flow and avoid
inadvertent reflux of Onyx into the ICA. (f, g, h) A radical occlusion
of DAVF, preserving the patency of the ophthalmic artery. (i) No filling
of DAVF from the ECA.
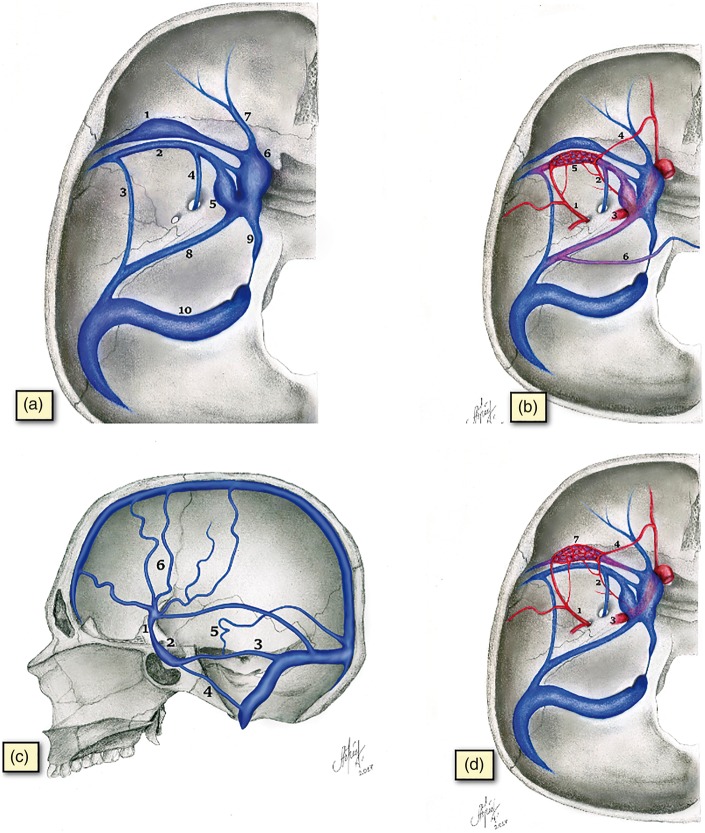
Topographical and anatomical relationships between venous structures in
the lesser sphenoid wing region. Normal venous drainage vs. in presence
of an arteriovenous fistula (AV-fistula). (a) The anatomy of the venous
system in the lesser sphenoid wing region and normal venous drainage
pathways. (1) Dural sinus of the lesser sphenoid wing. (2) Superficial
middle cerebral vein. (3) An example of SMCV drainage into the superior
petrosal sinus (sphenopetrosal sinus). (4) An example of SMCV drainage
into the pterygopalatine plexus through the foramen rotundum. (5)
Paracavernous sinus. (6) Cavernous sinus. (7) Superior orbital vein. (8)
Superior petrosal sinus. (9) Inferior petrosal sinus. (10) Sigmoid
sinus. (b) AV-fistula of the superficial middle cerebral vein. (1)
Middle meningeal artery. (2) Branches of the inferolateral trunk of the
internal carotid artery (ICA). (3) The ICA. (4) Recurrent meningeal
branch of the ophthalmic artery. (5) AV-fistula of superficial middle
cerebral vein. (6) Venous drainage into the basal veins via the lateral
mesencephalic and peduncular veins to the opposite vein of Rosenthal.
(7) AV-fistula in the sinus region of the lesser sphenoid wing. (c)
Venous drainage pathways of arteriovenous fistula of the superficial
middle cerebral vein. (1) Superficial middle cerebral vein. (2)
Cavernous sinus. (3) Superior petrosal sinus. (4) Inferior petrosal
sinus. (5) Venous drainage into the deep veins of the brain. (6)
Drainage into the superficial cortical veins. (d) AV-fistula of the
lesser sphenoid wing. (1) Middle meningeal artery. (2) Branches of the
inferolateral trunk of the ICA. (3) The ICA. (4) Recurrent meningeal
branch of the ophthalmic artery. (5) AV-fistula of superficial middle
cerebral vein. (6) Venous drainage into the basal veins via the lateral
mesencephalic and peduncular veins to the opposite vein of Rosenthal.
(7) AV-fistula in the sinus region of the lesser sphenoid wing.
References
-
- Cognard C, Gobin YP, Pierot L, et al. Cerebral dural arteriovenous fistulas: Clinical and angiographic correlation with a revised classification of venous drainage. Radiology 1995; 194: 671–680. - PubMed
-
- Bitoh S, Arita N, Fujiwara M, et al. Dural arteriovenous malformation near the left sphenoparietal sinus. Surg Neurol 1980; 13: 345–349. - PubMed
-
- Tsutsumi K, Shiokawa Y, Kubota M, et al. Postoperative arteriovenous fistula between the middle meningeal artery and sphenoparietal sinus. Neurosurgery 1990; 26: 869–870. - PubMed
-
- Ezura M, Takahashi A, Mizoi K. Dural arteriovenous shunts involving the sphenoparietal sinus. A case report. Interv Neuroradiol 1996; 2: 223–228. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
