

Thyroid Nodules with Indeterminate Cytology: Utility of the American Thyroid Association Sonographic Patterns for Cancer Risk Stratification
- PMID: 29848195
- PMCID: PMC6916126
- DOI: 10.1089/thy.2018.0085
Thyroid Nodules with Indeterminate Cytology: Utility of the American Thyroid Association Sonographic Patterns for Cancer Risk Stratification
Abstract
Background: The 2015 American Thyroid Association (ATA) guidelines recommend using a classification based on sonographic patterns to set the size threshold for biopsies. Each pattern is associated with a distinct estimated rate of malignancy that it was hypothesized should stratify the risk of malignancy of cytologically indeterminate thyroid nodules (ITNs).
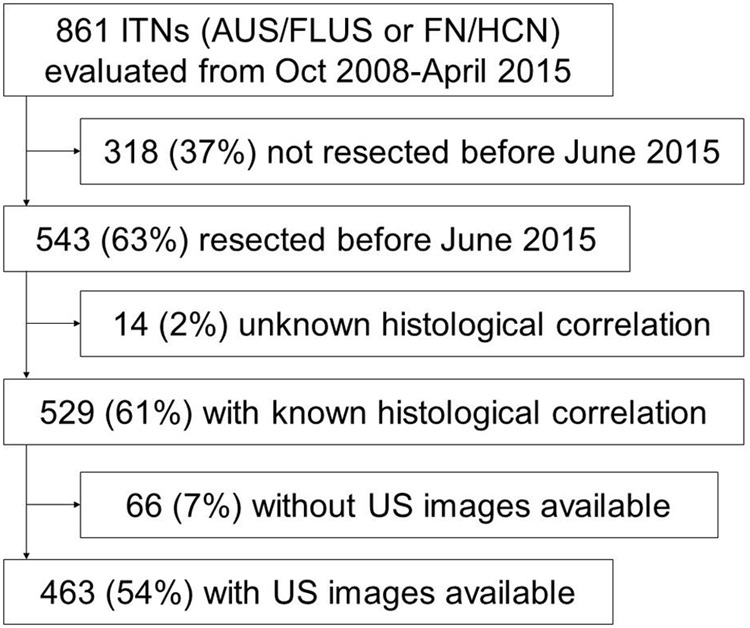
Methods: Ultrasound images of 463 ITNs (38% atypia/follicular lesions of undetermined significance; 62% follicular neoplasms) with histological follow-up consecutively evaluated between October 2008 and June 2015 at the authors' academic cancer center were independently evaluated by three observers and classified into one of the five sonographic patterns proposed by the ATA. Nodules with sonographic patterns not defined in the classification were grouped into a non-ATA pattern category. Differences in clinical and histological findings between the sonographic patterns were assessed. The prevalence of malignancy and odds ratio for malignancy were calculated for each sonographic pattern (low and intermediate patterns were collapsed for the analysis).
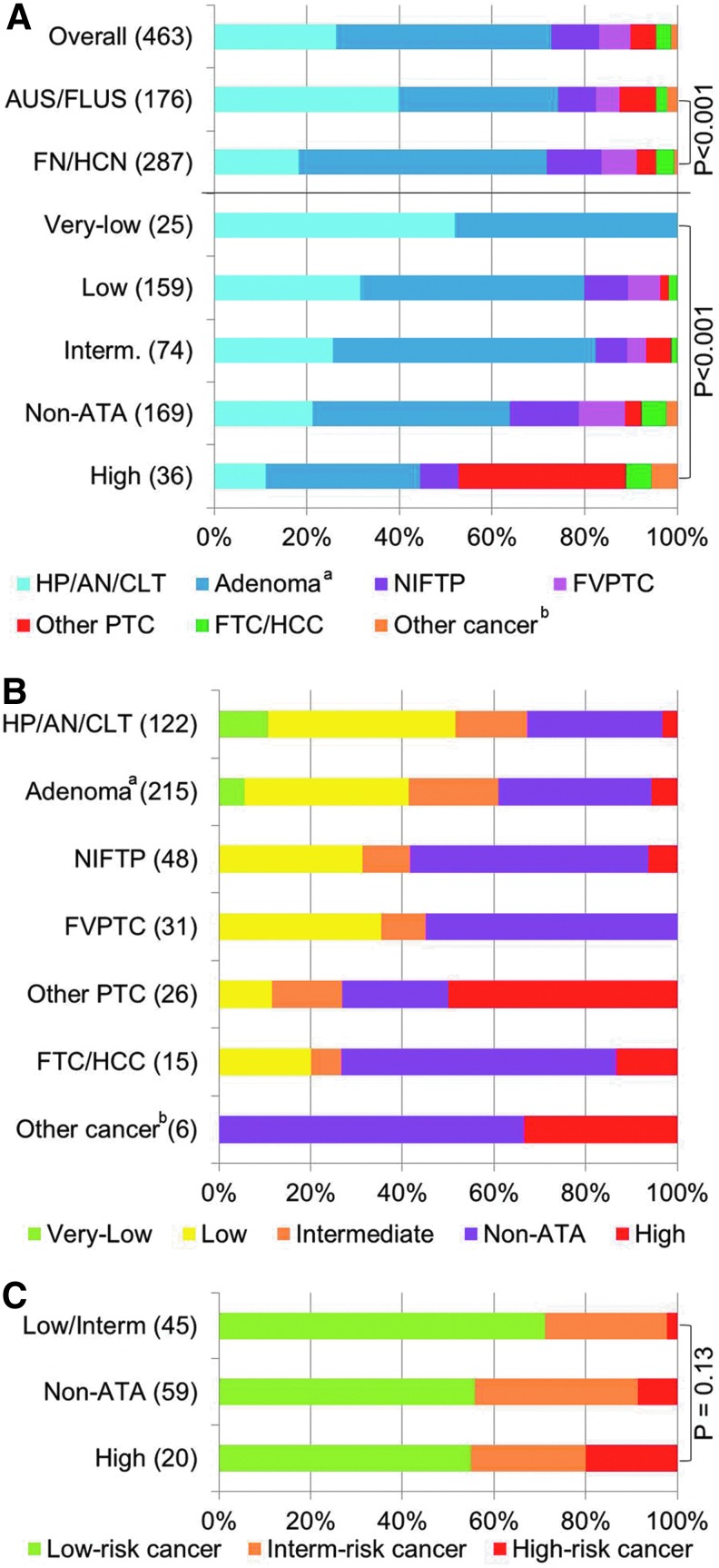
Results: The distribution of size and cytological diagnosis was significantly different between sonographic patterns (p < 0.001). The overall rate of malignancy was 27%. The rate of malignancy for the very low, low/intermediate, high, and non-ATA patterns were 0%, 19%, 56%, and 36%, respectively, and were all significantly different. Compared to the low/intermediate suspicion patterns, the odds ratios for malignancy were 2.35 for the non-ATA and 5.18 for the high suspicion patterns (p < 0.001). The odds ratio of the non-ATA pattern was 0.45 over the high suspicion pattern (p = 0.04). Results were similar in both cytological categories and for each observer separately. Sonographic patterns were associated with distinct histopathological profiles (p < 0.001).
Conclusions: ATA sonographic patterns are associated with distinct clinical features and pathological outcomes, and effectively stratify the cancer risk in ITNs. Thus, the ATA sonographic patterns should be used not only to set the size threshold for biopsy, but also to personalize management after the biopsy.
Keywords: noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP); thyroid cancer; thyroid cytology; thyroid nodules; thyroid ultrasound.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger M, Schuff KG, Sherman SI, Sosa JA, Steward DL, Tuttle RM, Wartofsky L. 2016. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 26:1–133 - PMC - PubMed
-
- Gharib H, Papini E, Garber JR, Duick DS, Harrell RM, Hegedus L, Paschke R, Valcavi R, Vitti P; AACE/ACE/AME Task Force on Thyroid Nodules 2016. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid modules—2016 update. Endocr Pract 22:622–639 - PubMed
-
- Perros P, Boelaert K, Colley S, Evans C, Evans RM, Gerrard Ba G, Gilbert J, Harrison B, Johnson SJ, Giles TE, Moss L, Lewington V, Newbold K, Taylor J, Thakker RV, Watkinson J, Williams GR. 2014. Guidelines for the management of thyroid cancer. Clin Endocrinol 81:1–122 - PubMed
-
- National Comprehensive Cancer Network 2017 NCCN Clinical Practice Guidelines in Oncology (NCCN guidelines). Thyroid Carcinoma (version 2.2017). Available at: www.nccn.org/professionals/physician_gls/f_guidelines.asp#thyroid (accessed June30, 2017)
-
- Bongiovanni M, Spitale A, Faquin WC, Mazzucchelli L, Baloch ZW. 2012. The Bethesda System for Reporting Thyroid Cytopathology: a meta-analysis. Acta Cytol 56:333–339 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
