

Para-duodenal hernia: a report of five cases and review of literature
- PMID: 29848337
- PMCID: PMC5977483
- DOI: 10.1186/s12893-018-0365-8
Para-duodenal hernia: a report of five cases and review of literature
Abstract
Background: Para-duodenal hernia (PDH) represents rare clinical entities based on few literatures.
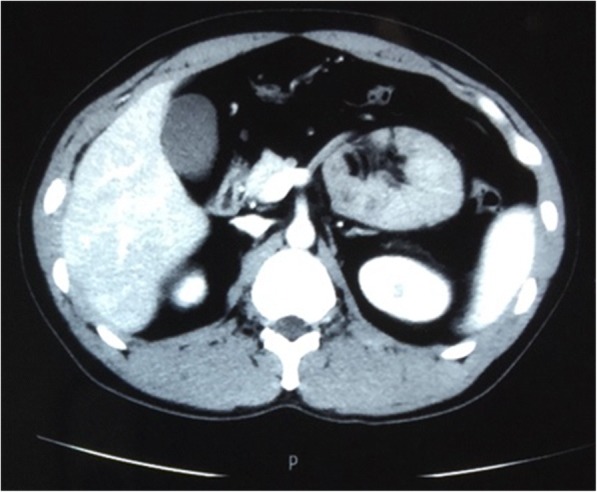
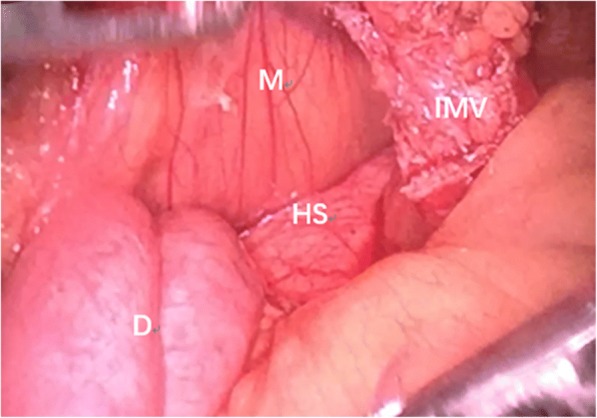
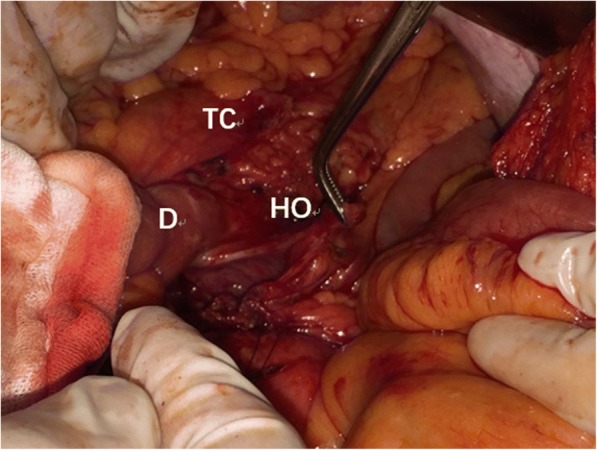
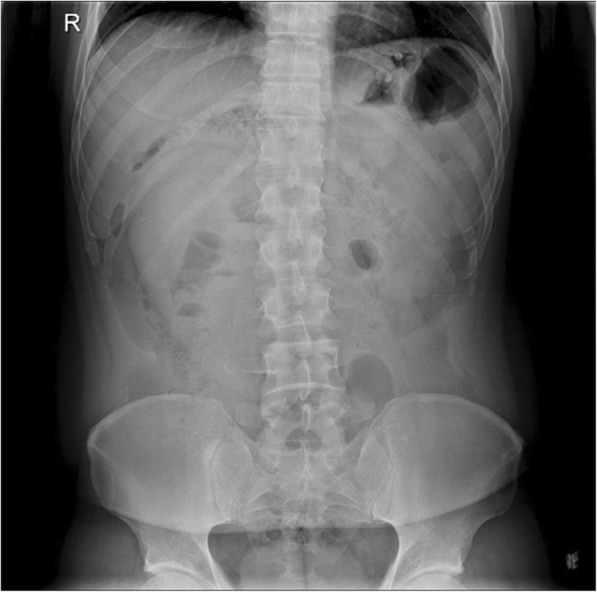
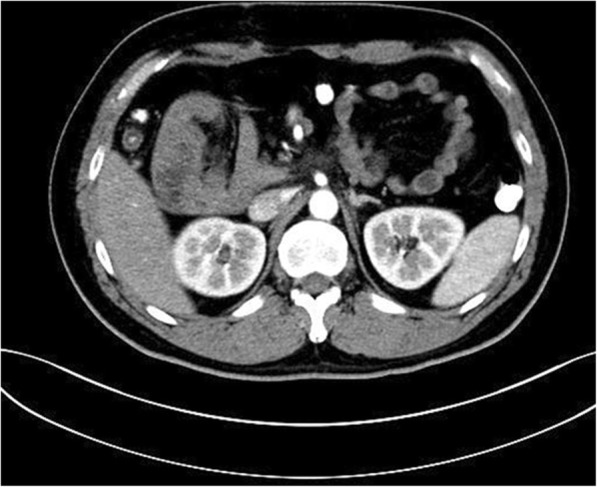
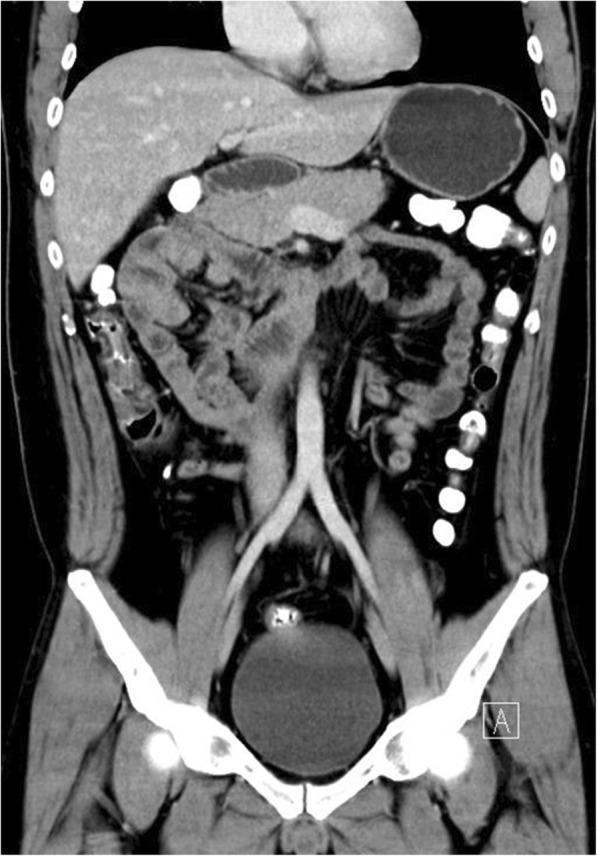
Case presentation: We report five cases of Para-duodenal hernia, all occurring in male patients ranging from 34 to 75 years of age. The patients had varied manifestations presenting with abdominal pain with or without vomiting and nausea and with or without signs of intestinal obstruction. CT images showed cluster of dilated bowel segments with displaced mesenteric vessels at hernial orifice. Laparoscopic surgical approach was adopted, and the patients were discharged about a week later without further complications.
Conclusion: We hope to raise awareness about the management of this rare clinical entity and the benefits of CT imaging and laparoscopic surgery as standard approaches.
Keywords: Abdominal pain; CT images; Intestinal obstruction; Laparoscopic surgery; Paraduodenal hernia.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the participants for publication of this article and any accompanying tables/images. A copy of the written consent is available for review by the Editor of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures







References
-
- Khan MA, Lo AY, Vande Maele DM. Paraduodenal hernia. Am Surg. 1998;64(12):1218–1222. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
