

School-Based versus Community-Based Sampling for Trachoma Surveillance
- PMID: 29848403
- PMCID: PMC6085813
- DOI: 10.4269/ajtmh.17-0904
School-Based versus Community-Based Sampling for Trachoma Surveillance
Abstract
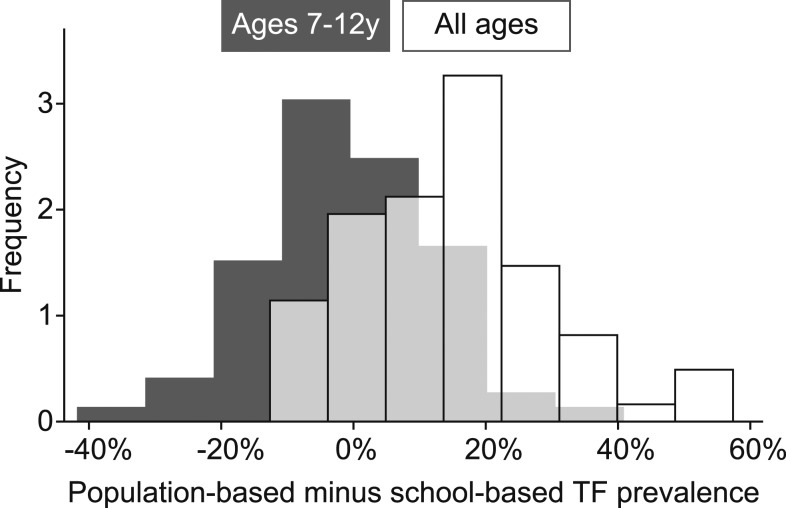
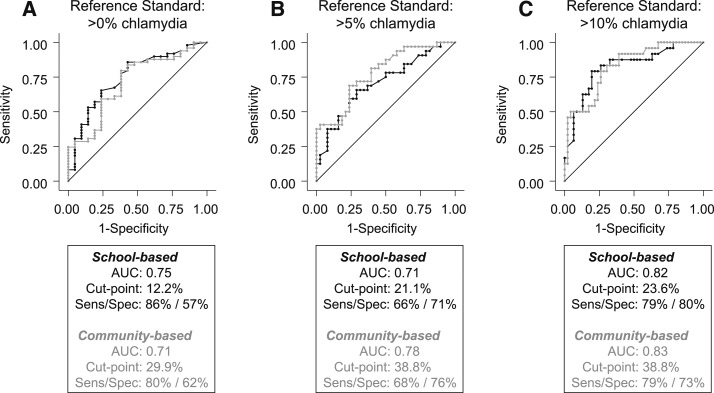
Trachoma surveillance is typically performed via random sampling of endemic districts. This strategy minimizes bias and allows examination of preschool children, but is also expensive. Surveillance for some other neglected tropical diseases is carried out in schools, which is logistically easier. In the present study, the prevalence of trachomatous inflammation-follicular (TF) from a population-based sample of children from each of 70 communities in Ethiopia was compared with the corresponding school-based estimate, which was calculated for each community by performing examinations in all primary schools in the district. The overall prevalence of TF was 39.1% (95% confidence interval [CI]: 35.0-43.1%) among children aged 1-9 years in the community-based sample and 18.8% (95% CI: 15.9-21.7%) among children in grades 1-3 of the school-based sample. School-based estimates of TF explained 35% of the variation in the community-based prevalences (P < 0.001). When TF prevalence was used as a diagnostic test for detecting a community with > 5% prevalence of ocular chlamydia, the area under the receiver operating characteristic curve was 0.73 (95% CI: 0.60-0.85) for the school-based sample and 0.71 (0.58-0.83) for the community-based sample (P = 0.76). Thus, although school-based monitoring was necessarily biased relative to population-based monitoring of 1- to 9-year olds, the two methods provided a similar amount of information about the community burden of ocular chlamydia in this trachoma-hyperendemic setting. The generalizability of these findings to areas with less prevalent trachoma is unclear.
Figures

References
-
- World Health Organization Strategic and Technical Advisory Group on Neglected Tropical Diseases , 2015. Technical Consultation on Trachoma Surveillance. Geneva, Switzerland: WHO.
-
- World Health Organization , 2015. Assessing the Epidemiology of Soil-Transmitted Helminths during a Transmission Assessment Survey in the Global Programme for the Elimination of Lymphatic Filariasis. Geneva, Switzerland: WHO.
-
- WHO Expert Committee , 2002. Prevention and control of schistosomiasis and soil-transmitted helminthiasis. World Health Organ Tech Rep Ser 912: 1–57 (back cover). - PubMed
-
- Solomon AW, et al. 2003. Strategies for control of trachoma: observational study with quantitative PCR. Lancet 362: 198–204. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
