

Prospective Analysis of Adoptive TIL Therapy in Patients with Metastatic Melanoma: Response, Impact of Anti-CTLA4, and Biomarkers to Predict Clinical Outcome
- PMID: 29848573
- PMCID: PMC6139043
- DOI: 10.1158/1078-0432.CCR-17-3649
Prospective Analysis of Adoptive TIL Therapy in Patients with Metastatic Melanoma: Response, Impact of Anti-CTLA4, and Biomarkers to Predict Clinical Outcome
Abstract
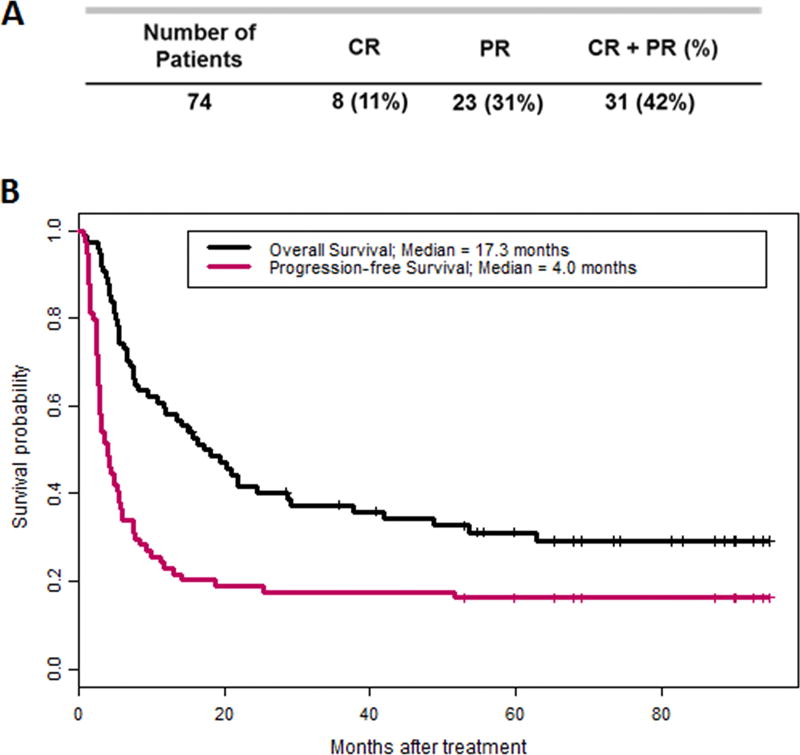
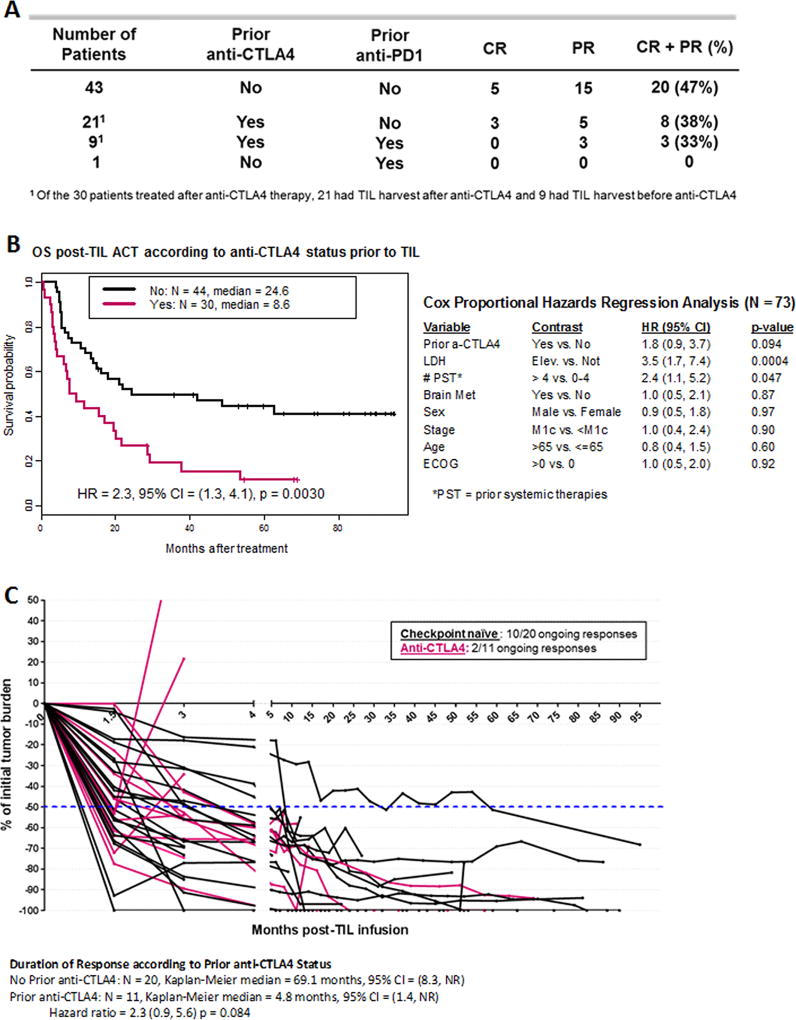
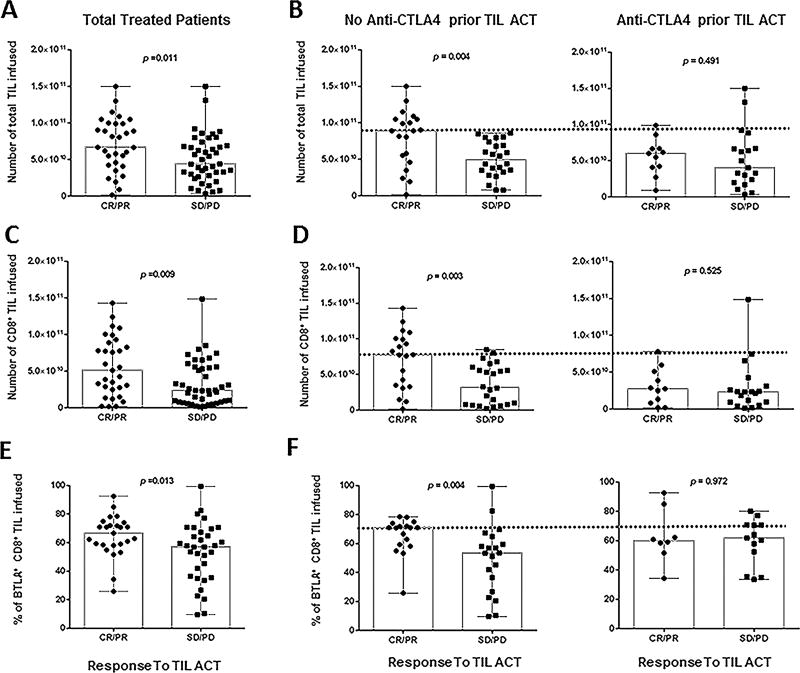
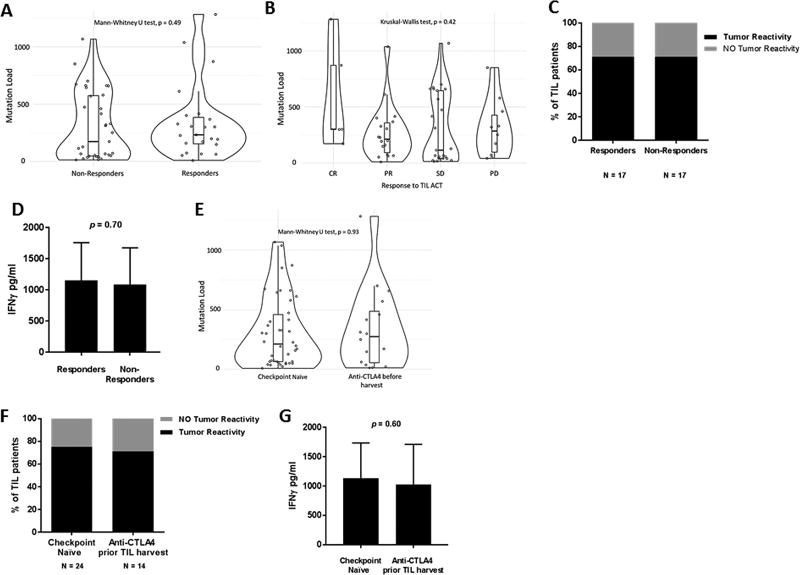
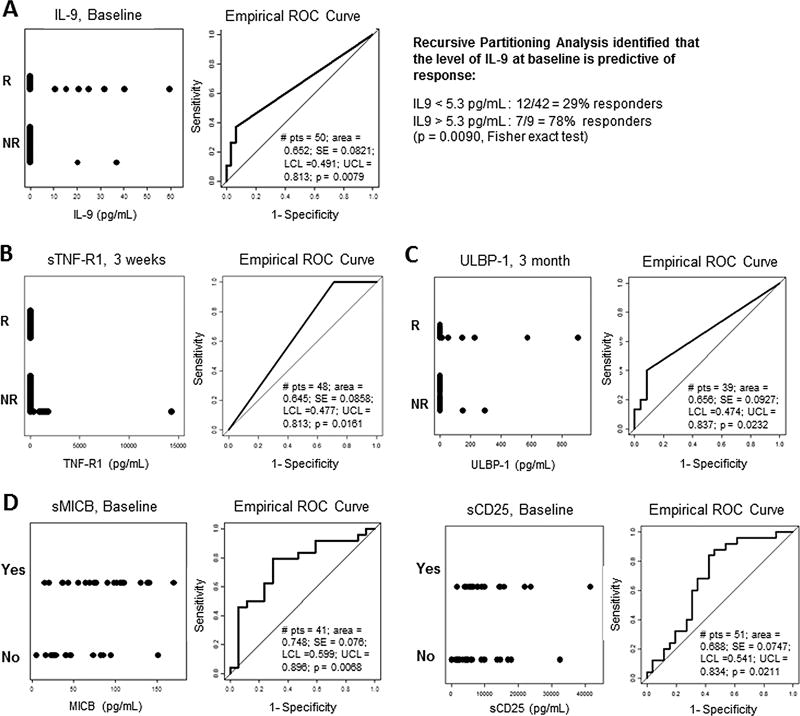
Purpose: Adoptive cell therapy (ACT) using tumor-infiltrating lymphocytes (TIL) has consistently demonstrated clinical efficacy in metastatic melanoma. Recent widespread use of checkpoint blockade has shifted the treatment landscape, raising questions regarding impact of these therapies on response to TIL and appropriate immunotherapy sequence.Patients and Methods: Seventy-four metastatic melanoma patients were treated with autologous TIL and evaluated for clinical response according to irRC, overall survival, and progression-free survival. Immunologic factors associated with response were also evaluated.Results: Best overall response for the entire cohort was 42%; 47% in 43 checkpoint-naïve patients, 38% when patients were exposed to anti-CTLA4 alone (21 patients) and 33% if also exposed to anti-PD1 (9 patients) prior to TIL ACT. Median overall survival was 17.3 months; 24.6 months in CTLA4-naïve patients and 8.6 months in patients with prior CTLA4 blockade. The latter patients were infused with fewer TIL and experienced a shorter duration of response. Infusion of higher numbers of TIL with CD8 predominance and expression of BTLA correlated with improved response in anti-CTLA4 naïve patients, but not in anti-CTLA4 refractory patients. Baseline serum levels of IL9 predicted response to TIL ACT, while TIL persistence, tumor recognition, and mutation burden did not correlate with outcome.Conclusions: This study demonstrates the deleterious effects of prior exposure to anti-CTLA4 on TIL ACT response and shows that baseline IL9 levels can potentially serve as a predictive tool to select the appropriate sequence of immunotherapies. Clin Cancer Res; 24(18); 4416-28. ©2018 AACR.
©2018 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Radvanyi LG, Bernatchez C, Zhang M, Fox PS, Miller P, Chacon J, et al. Specific lymphocyte subsets predict response to adoptive cell therapy using expanded autologous tumor-infiltrating lymphocytes in metastatic melanoma patients. Clin Cancer Res. 2012;18(24):6758–70. doi: 10.1158/1078-0432.CCR-12-1177. - DOI - PMC - PubMed
-
- Besser MJ, Shapira-Frommer R, Itzhaki O, Treves AJ, Zippel DB, Levy D, et al. Adoptive transfer of tumor-infiltrating lymphocytes in patients with metastatic melanoma: intent-to-treat analysis and efficacy after failure to prior immunotherapies. Clin Cancer Res. 2013;19(17):4792–800. doi: 10.1158/1078-0432.CCR-13-0380. - DOI - PubMed
-
- Andersen R, Donia M, Ellebaek E, Borch TH, Kongsted P, Iversen TZ, et al. Long-lasting complete responses in patients with metastatic melanoma after adoptive cell therapy with tumor-infiltrating lymphocytes and an attenuated IL-2 regimen. Clin Cancer Res. 2016 doi: 10.1158/1078-0432.CCR-15-1879. - DOI - PubMed
-
- Goff SL, Dudley ME, Citrin DE, Somerville RP, Wunderlich JR, Danforth DN, et al. Randomized, Prospective Evaluation Comparing Intensity of Lymphodepletion Before Adoptive Transfer of Tumor-Infiltrating Lymphocytes for Patients With Metastatic Melanoma. J Clin Oncol. 2016;34(20):2389–97. doi: 10.1200/JCO.2016.66.7220. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
