

Restarting antiplatelet therapy after spontaneous intracerebral hemorrhage: Functional outcomes
- PMID: 29848784
- PMCID: PMC6091879
- DOI: 10.1212/WNL.0000000000005742
Restarting antiplatelet therapy after spontaneous intracerebral hemorrhage: Functional outcomes
Abstract
Objective: To compare the functional outcomes and health-related quality of life metrics of restarting vs not restarting antiplatelet therapy (APT) in patients presenting with intracerebral hemorrhage (ICH) in the ERICH (Ethnic/Racial Variations of Intracerebral Hemorrhage) study.
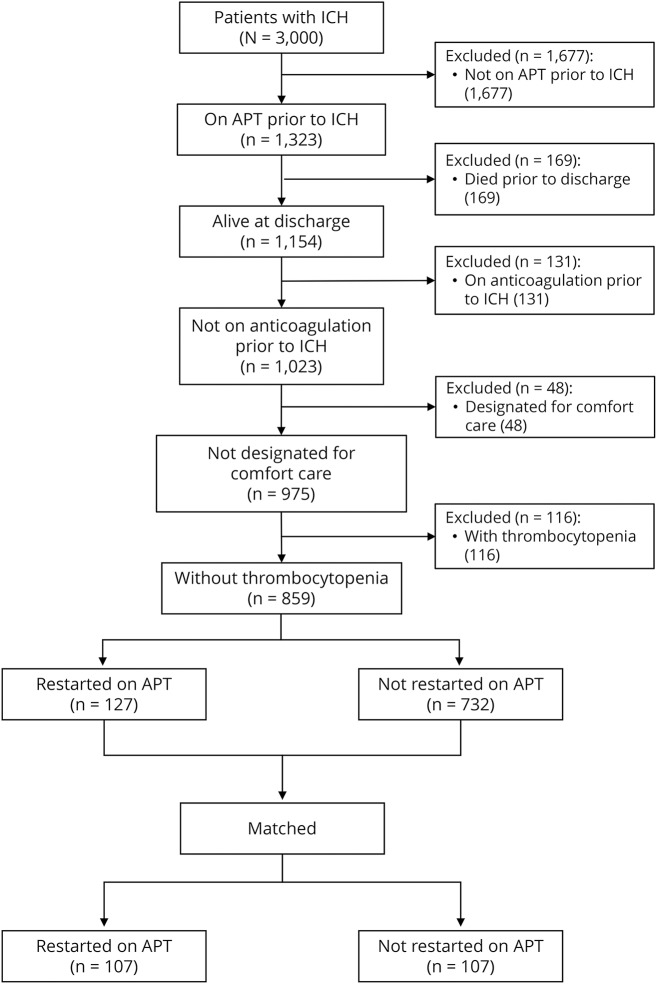
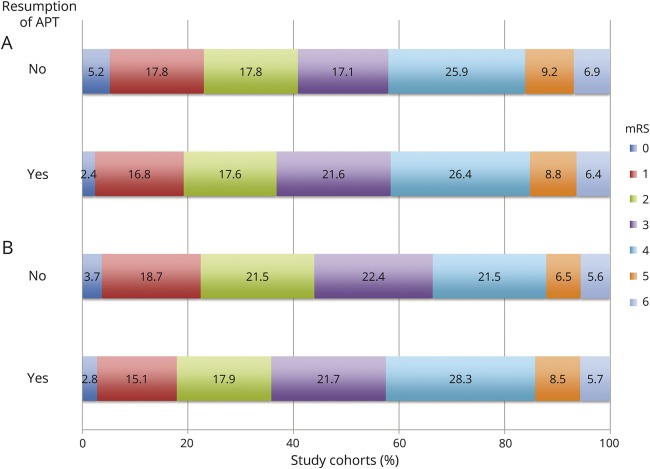
Methods: Adult patients aged 18 years and older who were on APT before ICH and were alive at hospital discharge were included. Patients were dichotomized based on whether or not APT was restarted after hospital discharge. The primary outcome was a modified Rankin Scale score of 0-2 at 90 days. Secondary outcomes were excellent outcome (modified Rankin Scale score 0-1), mortality, Barthel Index, and health status (EuroQol-5 dimensions [EQ-5D] and EQ-5D visual analog scale scores) at 90 days.
Results: The APT and no APT cohorts comprised 127 and 732 patients, respectively. Restarting APT was associated with lower rates of good functional outcome (36.5% vs 40.8%; p = 0.021) and lower Barthel Index scores at 90 days (p = 0.041). The 2 cohorts were then matched in a 1:1 ratio, and the matched cohorts each comprised 107 patients. No difference in primary outcome was observed between restarting vs not restarting APT (35.5% vs 43.9%; p = 0.105). There were also no differences between the secondary outcomes of the 2 cohorts.
Conclusion: Restarting APT in patients with ICH of mild to moderate severity after acute hospitalization is not associated with worse functional outcomes or health-related quality of life at 90 days. In patients with significant cardiovascular risk factors who experience an ICH, restarting APT remains the decision of the treating practitioner.
© 2018 American Academy of Neurology.
Figures
References
-
- He J, Whelton PK, Vu B, Klag MJ. Aspirin and risk of hemorrhagic stroke: a meta-analysis of randomized controlled trials. JAMA 1998;280:1930–1935. - PubMed
-
- Ducrocq G, Amarenco P, Labreuche J, et al. A history of stroke/transient ischemic attack indicates high risks of cardiovascular event and hemorrhagic stroke in patients with coronary artery disease. Circulation 2013;127:730–738. - PubMed
-
- Khan NI, Siddiqui FM, Goldstein JN, et al. Association between previous use of antiplatelet therapy and intracerebral hemorrhage outcomes. Stroke 2017;48:1810–1817. - PubMed
-
- Ottosen TP, Grijota M, Hansen ML, et al. Use of antithrombotic therapy and long-term clinical outcome among patients surviving intracerebral hemorrhage. Stroke 2016;47:1837–1843. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources