

Clinical characteristics and diagnosis of a rare case of systemic AL amyloidosis: a descriptive study
- PMID: 29849940
- PMCID: PMC5966272
- DOI: 10.18632/oncotarget.25055
Clinical characteristics and diagnosis of a rare case of systemic AL amyloidosis: a descriptive study
Abstract
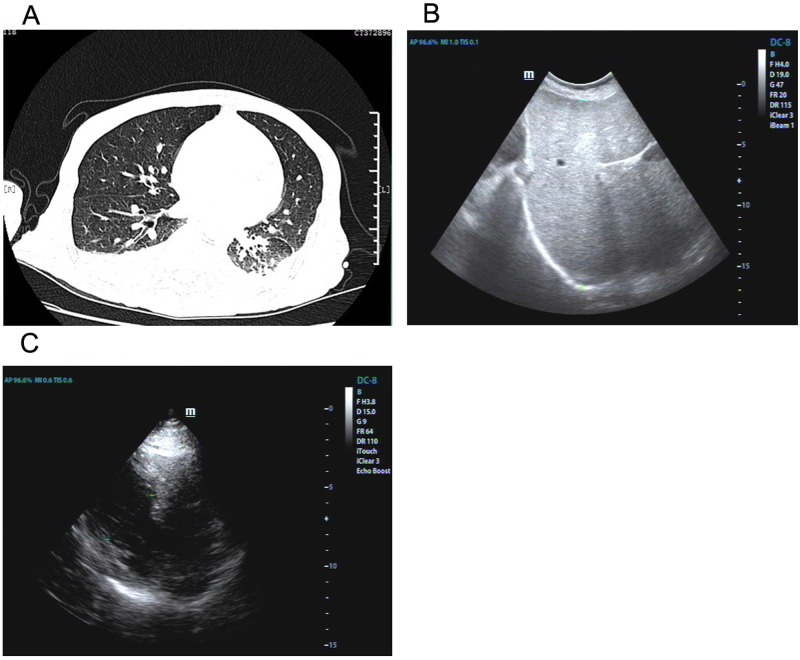
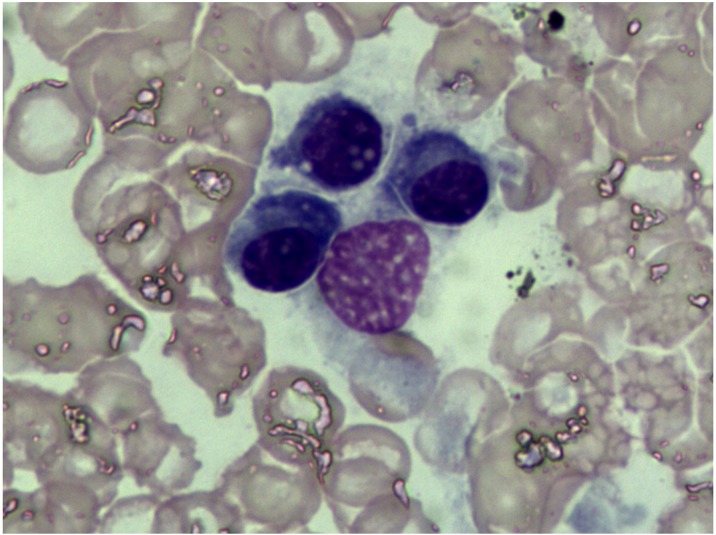
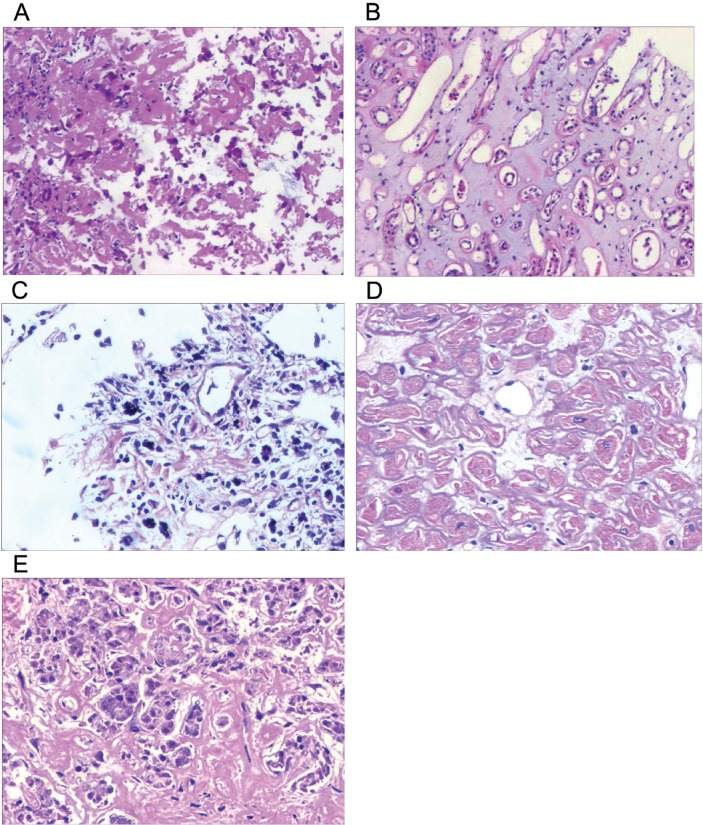
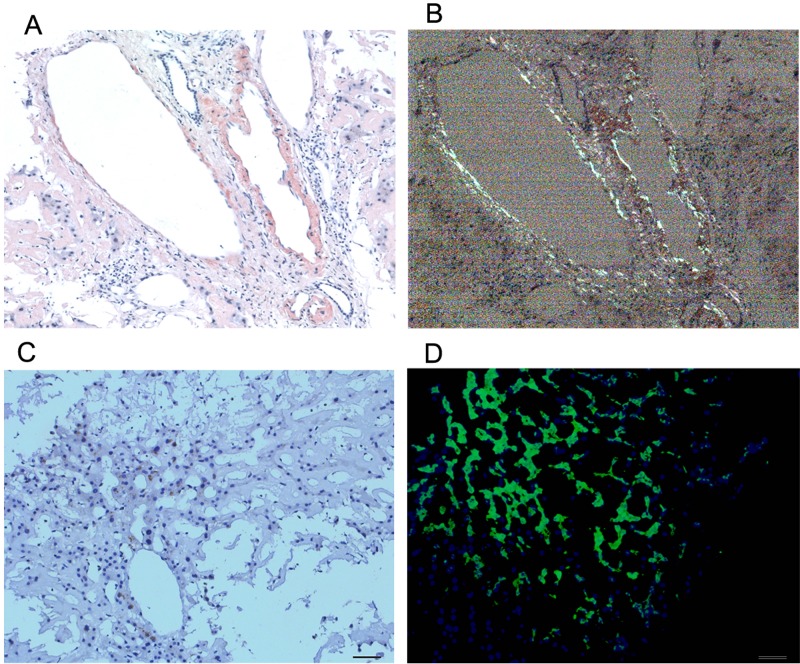
Systemic amyloidosis is a rare disease involving multiple organs. It is difficult to establish diagnosis as the symptoms is diverse and non-specific. And without specific therapy the prognosis is very poor. We analyzed detailed clinical and laboratorial data of a 53-year-old male patient. The characteristic features included refractory pleural effusion, extraordinary hepatomegaly and cardiac failure. The illness lasted 9 months and therapy period spanned 4 months. Fine needle biopsy of liver, lung, heart, pancreas and kidney was performed. Immunohistochemistry, immunofluorescence, Congo staining and hematoxylin and eosin staining were performed. All specimens were stained pink with haematoxylin and eosin staining. Amorphous deposits of eosinophilic material were visible within the Congo red dye stained liver tissue whereas under cross-polarized light pathognomonic apple-green birefringence of amyloid deposits was visible. At last systemic AL amyloidosis diagnosis was confirmed. The report showed an unusual AL amyloidosis case in detail which would be helpful for physician in clinical work.
Keywords: amyloidosis; hepatomegaly.
Conflict of interest statement
CONFLICTS OF INTEREST There is no conflicts of interest.
Figures
Similar articles
-
Digitally reinforced polarization of hematoxylin-eosin in the diagnosis of renal amyloidosis.Turk Patoloji Derg. 2012;28(3):204-12. doi: 10.5146/tjpath.2012.01126. Turk Patoloji Derg. 2012. PMID: 23011822
-
Amyloidosis diagnosed in cytology specimen of pleural effusion: A case report.Diagn Cytopathol. 2018 Jun;46(6):522-524. doi: 10.1002/dc.23877. Epub 2017 Dec 27. Diagn Cytopathol. 2018. PMID: 29280335
-
Diagnosis of pulmonary amyloidosis by transbronchial biopsy.Am Rev Respir Dis. 1985 Jul;132(1):191-4. doi: 10.1164/arrd.1985.132.1.191. Am Rev Respir Dis. 1985. PMID: 4014866
-
Cardiac Amyloidosis.Heart Fail Clin. 2022 Jul;18(3):479-488. doi: 10.1016/j.hfc.2022.02.005. Heart Fail Clin. 2022. PMID: 35718420 Free PMC article. Review.
-
Nodular goiter with amyloid deposition in an elderly patient: fine-needle cytology diagnosis and review of the literature.BMC Surg. 2013;13 Suppl 2(Suppl 2):S43. doi: 10.1186/1471-2482-13-S2-S43. Epub 2013 Oct 8. BMC Surg. 2013. PMID: 24267036 Free PMC article. Review.
Cited by
-
Characteristics of pleural effusion due to amyloidosis.Ann Thorac Med. 2023 Apr-Jun;18(2):53-60. doi: 10.4103/atm.atm_433_22. Epub 2023 Apr 25. Ann Thorac Med. 2023. PMID: 37323369 Free PMC article. Review.
-
Evaluation of laboratory diagnostic tests for light-chain clonality and bone marrow findings in AL amyloidosis.Blood Res. 2023 Mar 31;58(1):71-76. doi: 10.5045/br.2023.2022232. Blood Res. 2023. PMID: 36987618 Free PMC article.
-
Amyloid Proteins and Peripheral Neuropathy.Cells. 2020 Jun 26;9(6):1553. doi: 10.3390/cells9061553. Cells. 2020. PMID: 32604774 Free PMC article. Review.
References
-
- Wechalekar AD, Gillmore JD, Hawkins PN. Systemic amyloidosis. Lancet. 2016;387:2641–54. - PubMed
-
- Gillmore JD, Hawkins PN. Pathophysiology and treatment of systemic amyloidosis. Nat Rev Nephrol. 2013;9:574–86. - PubMed
-
- Dispenzieri A, Gertz MA, Kyle RA, Lacy MQ, Burritt MF, Therneau TM, Greipp PR, Witzig TE, Lust JA, Rajkumar SV, Fonseca R, Zeldenrust SR, McGregor CG, et al. Serum cardiac troponins and N-terminal pro-brain natriuretic peptide: a staging system for primary systemic amyloidosis. J Clin Oncol. 2004;22:3751–7. - PubMed
-
- Dember LM, Shepard JA, Nesta F, Stone JR. Case records of the Massachusetts General Hospital. Case 15-2005. An 80-year-old man with shortness of breath, edema, and proteinuria. N Engl J Med. 2005;352:2111–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
