

Cardiac radiation dose distribution, cardiac events and mortality in early-stage lung cancer treated with stereotactic body radiation therapy (SBRT)
- PMID: 29850140
- PMCID: PMC5949491
- DOI: 10.21037/jtd.2018.04.42
Cardiac radiation dose distribution, cardiac events and mortality in early-stage lung cancer treated with stereotactic body radiation therapy (SBRT)
Abstract
Background: The impact of radiation dose to the heart in early-stage lung cancer patients treated with definitive stereotactic body radiation therapy (SBRT) is not well known. We, therefore, analyzed whether higher radiation dose to the heart would lead to an increase in cardiac toxicity and overall mortality.
Methods: Seventy-four patients with 75 tumors treated definitively with SBRT for early-stage non-small cell lung cancer (NSCLC) and two cases of limited-stage small cell lung cancer (SCLC) with an average follow-up of 35 months (range, 1-130 months) were retrospectively analyzed. The whole heart and cardiac substructures including atria, ventricles, heart valves, atrioventricular (AV) node and four major coronary artery branches were contoured using commercial treatment planning software. For each structure, multiple dose-volume parameters were recorded. The relation between radiation doses to the heart, tumor location, and preexisting medical conditions with the development of cardiac events and mortality was assessed.
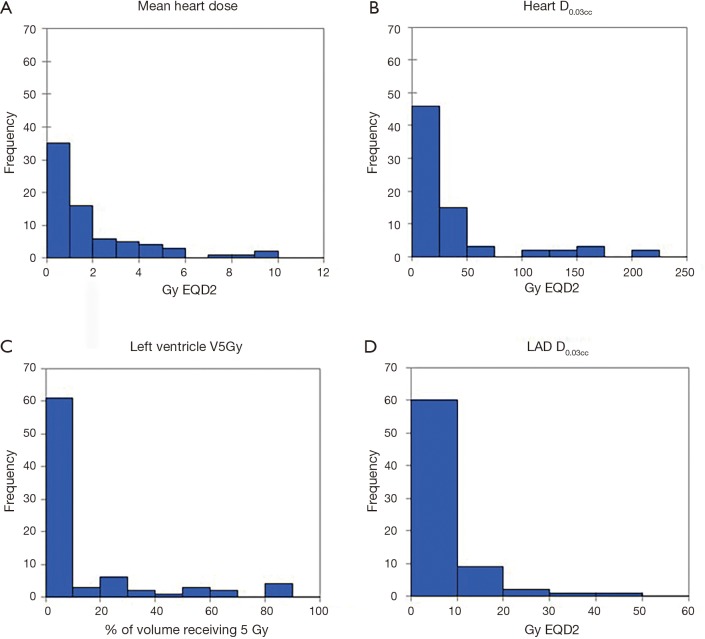
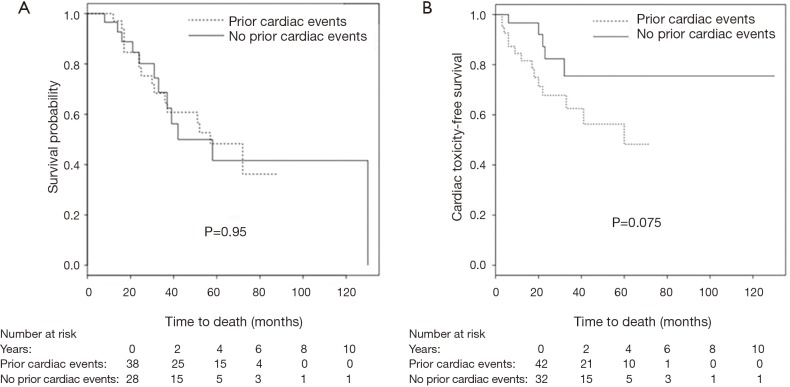
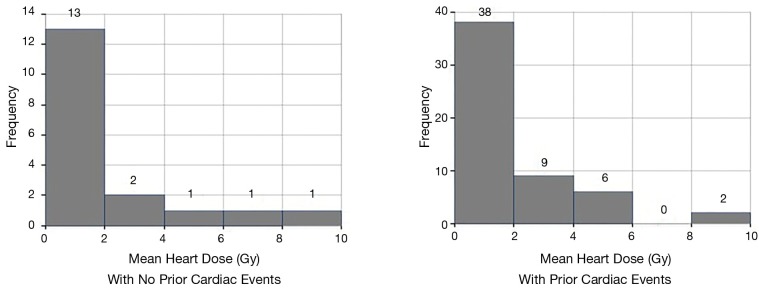
Results: Overall, there was large variability in dose to cardiac substructures: mean heart dose (MHD) averaged 1.90 Gy (range, 0.04-11.00 Gy) equivalent 2 Gy dose (EQD2) and average max dose to the left anterior descending artery (LAD) was 5.67 Gy (range, 0.04-48.60 Gy) EQD2. Patients with tumor location in the upper lobes received higher cardiac radiation dose compared to other lobes (P<0.0001). There was no difference in MHD between central and peripheral tumor locations. The distance between heart and tumor was negatively associated with MHD (r=-0.61, P<0.0001). Eighteen patients developed cardiac complications including the need for defibrillator placement, arrhythmia development and worsening heart failure. Preexisting cardiac disease was associated with an increased number of cardiac events after radiotherapy (P=0.039). However, neither radiation dose to the whole heart or the cardiac substructures, nor comorbidities such as diabetes, hypercholesterolemia, hypertension or COPD were associated with the number of cardiac events or overall mortality.
Conclusions: Radiation doses to the heart and its substructures show large variability. Cardiac events occurred more frequently in patients with a history of heart problems. At present, the effect of radiation dose on cardiac toxicity is unclear in patients undergoing SBRT for early-stage lung cancer. Longer follow-up and a larger cohort are needed to assess for late cardiac sequelae.
Keywords: Lung cancer; heart toxicity; stereotactic body radiation therapy (SBRT).
Conflict of interest statement
Conflicts of Interest: GD. Hugo: research funding Philips, NCI, license agreement Varian. E Weiss: research funding Philips and Varian Medical Systems, NCI, royalties from UpToDate. The other authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources