

Microwave Thermal Ablation in an Unusual Case of Malignant and Locally Advanced Rare Tumor of Pancreas in ASA IV Old Male Patient and Literature Review
- PMID: 29850295
- PMCID: PMC5925082
- DOI: 10.1155/2018/6064912
Microwave Thermal Ablation in an Unusual Case of Malignant and Locally Advanced Rare Tumor of Pancreas in ASA IV Old Male Patient and Literature Review
Abstract
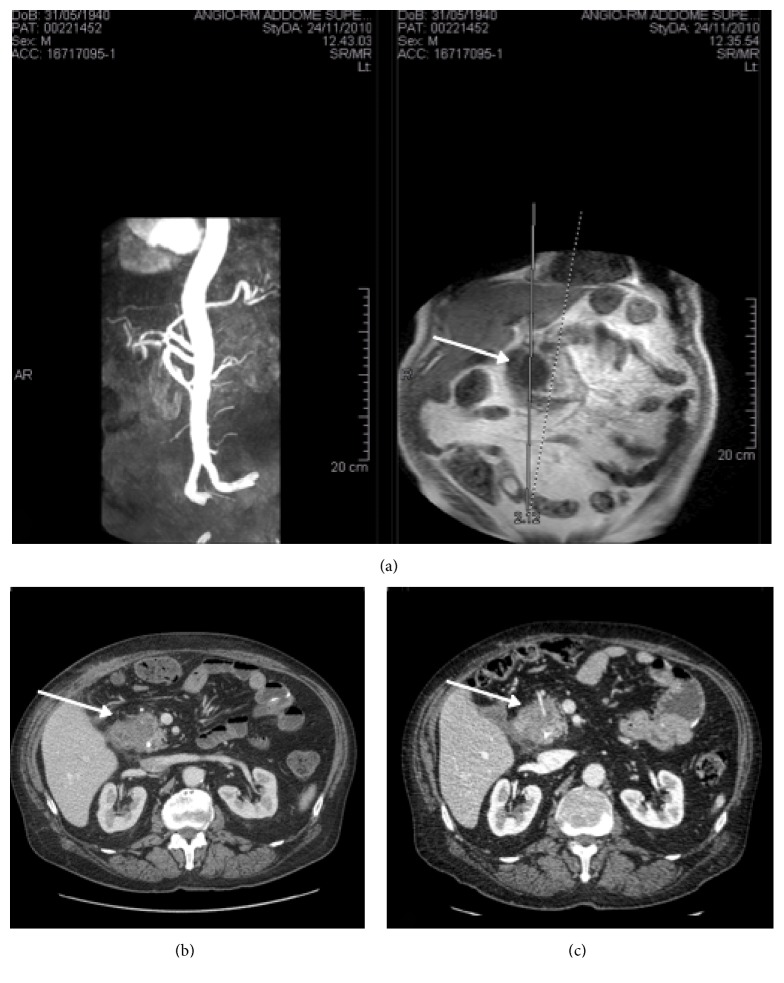
Pancreatic intraductal papillary-mucinous neoplasm is a rare primary neoplasm of unknown pathogenesis. This kind of tumor represents 0.2-2.7% of all pancreatic cancers and they may proceed to malignant lesions. In this study, we describe a case of pancreatic intraductal papillary-mucinous tumor (4.3 cm) with normal tumoral markers and nuclear atypia. We perform also a systematic review of the literature on MEDLINE and find only one relevant study that used microwave ablation for the palliative treatment of pancreatic tumor. We describe the case of a 70-year-old Caucasian male who was diagnosed with a pancreatic tumor with biliary tree dilatation. The patient underwent computed tomography (CT), percutaneous biopsy, and an endoscopic positioning of prosthesis in the biliary tree. Due to the worsening of jaundice and cholestasis, and considering the severe systemic disease status, palliative surgery with microwave thermoablation in the head of pancreas was performed. No complications were observed. The hospitalization lasted for 11 days after surgery, with normal liver and pancreatic lab tests at discharge. The patient followed a line of chemotherapy for 6 months with a complete response for 8 months. One month after the treatment, a staging CT scan was performed showing the size of the cephalopancreatic lesion had decreased from 43 to 35 mm with signs of complete ablation. The patient had a total response at the imaging of 10 months. One year later, a CT scan follow-up showed progression of the pancreatic disease. The disease remained stable for 18 months. The patient died due to cardiovascular complications with an overall survival of 30 months. Microwave ablation in our case report has been demonstrated to be feasible and safe without complications. It can be used as a phase of multimodality treatment in patients with severe systemic disease status and advanced intraductal papillary-mucinous neoplasm.
Figures
References
-
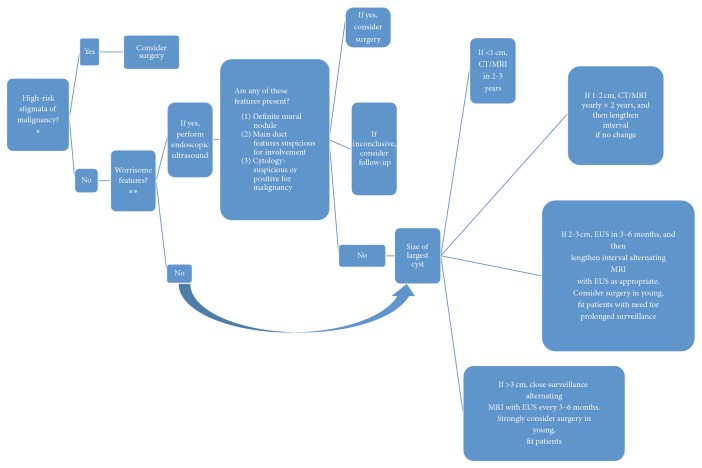
- Tanaka M., Chari S., Adsay V., et al. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology. 2006;6(1-2):17–32. - PubMed
-
- Salvia R., Fernández-Del Castillo C., Bassi C., et al. Main-duct intraductal papillary mucinous neoplasms of the pancreas: clinical predictors of malignancy and longterm survival following resection. Annals of Surgery. 2004;239(5):678–687. doi: 10.1097/01.sla.0000124386.54496.15. - DOI - PMC - PubMed
-
- Tang R. S., Weinberg B., Dawson D. W., et al. Evaluation of the Guidelines for Operative Management of Pancreatic Branch-Duct Intraductal Papillary Mucinous Neoplasm. Clinical Gastroenterology and Hepatology. 2008;6(7):815–819. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
