

Same Phenotype in Children with Growth Hormone Deficiency and Resistance
- PMID: 29850346
- PMCID: PMC5925024
- DOI: 10.1155/2018/5902835
Same Phenotype in Children with Growth Hormone Deficiency and Resistance
Abstract
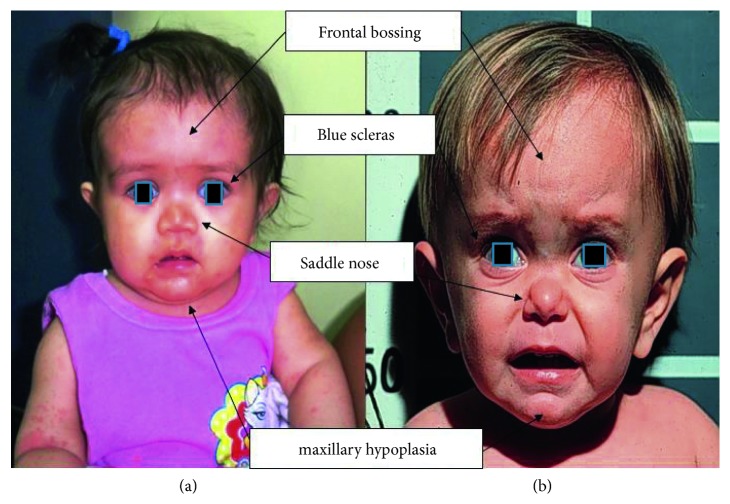
By definition, about 2.5% of children show a short stature due to several causes. Two clinical conditions are characterized by serum IGF-I low levels, idiopathic GH deficiency (IGHD), and GH insensitivity (GHI), and the phenotypic appearance of these patients may be very similar. We studied two children with short stature and similar phenotypes. The first case showed frontal bossing, doll face, acromicria, and truncal obesity, with a GH peak <0.05 ng/ml after stimuli and undetectable serum IGF-I levels. After PCR amplification of the whole GH1 gene, type IA idiopathic GHD was diagnosed. The second case had cranium hypoplasia, a large head, protruding forehead, saddle nose, underdeveloped mandible, and a micropenis. Basal GH levels were high (28.4 ng/ml) while serum IGF-I levels were low and unchangeable during the IGF-I generation test. Laron syndrome was confirmed after the molecular analysis of the GH receptor (GHR) gene. IGHD type IA and Laron syndrome is characterized by opposite circulating levels of GH, while both have reduced levels of IGF-I, with an overlapping clinical phenotype, lacking the effects of IGF-I on cartilage. These classical cases show the importance of differential diagnosis in children with severe short stature.
Figures
Similar articles
-
IGFs and IGFBPs in GH insensitivity.Endocr Dev. 2005;9:100-106. doi: 10.1159/000085760. Endocr Dev. 2005. PMID: 15879692 Review.
-
Clinical features and growth hormone receptor gene mutations of patients with Laron syndrome from a Chinese family.Zhongguo Dang Dai Er Ke Za Zhi. 2007 Aug;9(4):335-8. Zhongguo Dang Dai Er Ke Za Zhi. 2007. PMID: 17706034
-
Short stature and decreased insulin-like growth factor I (IGF-I)/growth hormone (GH)-ratio in an adult GH-deficient patient pointing to additional partial GH insensitivity due to a R179C mutation of the growth hormone receptor.Growth Horm IGF Res. 2007 Aug;17(4):307-14. doi: 10.1016/j.ghir.2007.03.001. Epub 2007 Apr 25. Growth Horm IGF Res. 2007. PMID: 17462934
-
Insulin-like growth factor binding protein-3 generation: an index of growth hormone insensitivity.Pediatr Res. 1996 May;39(5):849-55. doi: 10.1203/00006450-199605000-00018. Pediatr Res. 1996. PMID: 8726240
-
Compound heterozygosity for two GHR missense mutations in a patient affected by Laron Syndrome: a case report.Ital J Pediatr. 2017 Oct 12;43(1):94. doi: 10.1186/s13052-017-0411-7. Ital J Pediatr. 2017. PMID: 29025428 Free PMC article. Review.
Cited by
-
A 42-Year-Old Woman with Untreated Growth Hormone Insensitivity, Diabetic Retinopathy, and Gene Sequencing Identifies a Variant of Laron Syndrome.Am J Case Rep. 2019 May 14;20:689-696. doi: 10.12659/AJCR.913178. Am J Case Rep. 2019. PMID: 31086127 Free PMC article.
-
Isolated growth hormone deficiency type IA due to a novel GH1 variant: a case report.BMC Med Genomics. 2021 Sep 2;14(1):210. doi: 10.1186/s12920-021-01057-z. BMC Med Genomics. 2021. PMID: 34470639 Free PMC article.
-
Role of the GH-IGF1 axis on the hypothalamus-pituitary-testicular axis function: lessons from Laron syndrome.Endocr Connect. 2021 Aug 25;10(9):1006-1017. doi: 10.1530/EC-21-0252. Endocr Connect. 2021. PMID: 34319907 Free PMC article.
-
Isolated Growth Hormone Deficiency IA due to a Novel Homozygous Large Deletion ∼1.6 kb Spanning Exons 1-4 of GH1 Gene: A Case Report.Clin Case Rep. 2025 Feb 19;13(2):e70234. doi: 10.1002/ccr3.70234. eCollection 2025 Feb. Clin Case Rep. 2025. PMID: 39980897 Free PMC article.
References
-
- Savage M. O., Burren C. P., Rosenfeld R. G. The continuum of growth hormone-IGF-I axis defects causing short stature: diagnostic and therapeutic challenges. Clinical Endocrinology. 2010;72:721–728. - PubMed
-
- Murray P. G., Clayton P. E. Disorders of growth hormone in childhood. In: De Groot L. J., Chrousos G., Dungan K., et al., editors. Endotext. South Dartmouth, MA, USA: MDText.com, Inc.; 2000.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
