

Surgical Reconstruction to Allow Endovascular Access for Flow Diversion of Giant Cavernous Aneurysm: A Combined Approach
- PMID: 29850376
- PMCID: PMC5973504
- DOI: 10.7759/cureus.2381
Surgical Reconstruction to Allow Endovascular Access for Flow Diversion of Giant Cavernous Aneurysm: A Combined Approach
Abstract
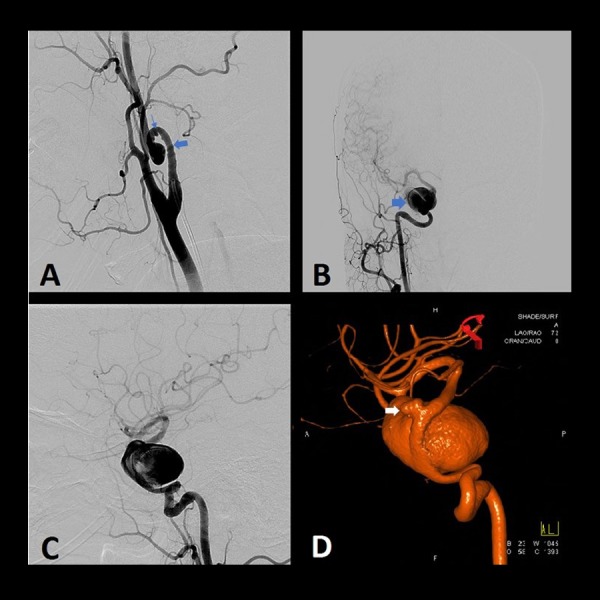
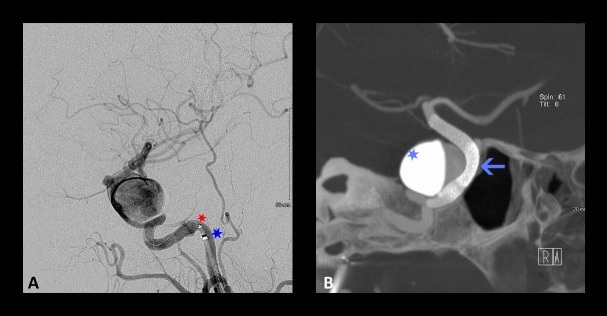
Giant cavernous aneurysms of the internal carotid artery (ICA) are challenging lesions associated with high surgical morbidity. Prior to the past several years, these were treated by surgical reconstruction, proximal ligation, or stent-assisted coiling techniques. Flow diversion has become the standard of care for these lesions, providing a high rate of obliteration with a much better safety profile. However, flow diverters rely upon a navigable vasculature and, usually, a tri-axial support system. Cases in which such access is difficult require unique approaches to combine the strengths of both surgical and endovascular therapy. A woman with a giant cavernous ICA aneurysm and an ophthalmic artery aneurysm presented for treatment, but access was challenging due to cervical ICA tortuosity and pseudoaneurysms. We elected a staged, combined approach with surgical reconstruction of the cervical ICA followed by flow diverter placement for the intracranial aneurysms. Our case features an "outside-the-box" approach that synergistically applied both microsurgical and endovascular techniques to treat a challenging pathology. Classic microsurgical techniques remain important in cases that are refractory or not amenable to endovascular therapy alone.
Keywords: carotid endarterectomy; cerebral aneurysm; cervical aneurysm; flow diversion; giant aneurysm; hunterian ligation.
Conflict of interest statement
Dr. Kan is a consultant for Medtronic and Styker.
Figures




References
-
- The expanding realm of endovascular neurosurgery: flow diversion for cerebral aneurysm management. Krishna C, Sonig A, Natarajan SK, Siddiqui AH. https://www.ncbi.nlm.nih.gov/pubmed/25624975. Methodist Debakey Cardiovasc J. 2014;10:214–219. - PMC - PubMed
-
- Earlier times in aneurysm surgery. Drake CG. Clin Neurosurg. 1985;32:41–50. - PubMed
-
- Cerebrovascular neurosurgery in evolution: the endovascular paradigm. Sorkin GC, Dumont TM, Eller JL, et al. Neurosurgery. 2014;74:191–197. - PubMed
-
- Reconstruction of the ligated external carotid artery for embolization of cervicofacial arteriovenous malformations. Riles TS, Berenstein A, Fisher FS, Persky MS, Madrid M. J Vasc Surg. 1993;17:491–498. - PubMed
-
- The combined approach to intracranial aneurysm treatment. Alexander BL, Riina HA. Surg Neurol. 2009;72:596–606. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous