

Evolving clinical applications of contrast-enhanced ultrasound (CEUS) in the abdominal aorta
- PMID: 29850424
- PMCID: PMC5949595
- DOI: 10.21037/cdt.2017.09.09
Evolving clinical applications of contrast-enhanced ultrasound (CEUS) in the abdominal aorta
Abstract
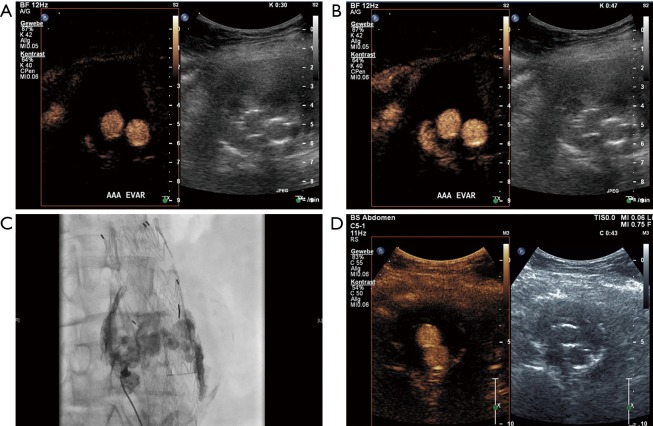
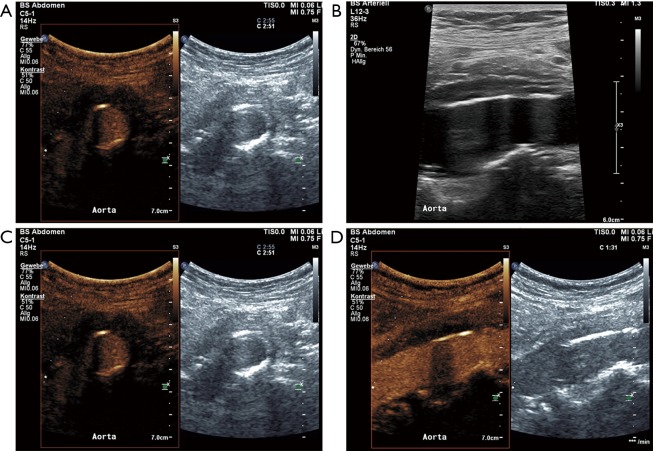
Ultrasound (US) represents the initial modality in the workup of abdominal aortic pathology based on the plethora of advantages including widespread availability, low cost, safety profile and repeatability. However, US has inherent limitations including limited spatial information of pathologic processes to neighboring structures, lower sensitivity to slow blood flow and aortic luminal irregularities. For evaluation of aortic pathology angiography has long been considered the gold standard. Non-invasive cross-sectional imaging techniques like computed tomography angiography (CTA) and magnetic resonance angiography (MRA) have gradually replaced interventional angiography for the evaluation of aorta, currently being regarded as the diagnostic imaging modalities of choice for diagnosis of virtually every aortic disease. Interventional angiography is currently primarily performed for treatment purposes of aortic pathology. The introduction of microbubbles as ultrasonographic contrast agents has rendered contrast-enhanced ultrasound (CEUS) an evolving valuable complementary technique with markedly increased diagnostic accuracy for certain aortic applications. CEUS is characterized by the potential to be performed in patients with impaired renal function. Due to its superior spatial and temporal resolution, ability for prolonged scanning and dynamic and real-time imaging, it provides clinically significant additional information compared to the standard Duplex US. The purpose of this paper is to discuss the currently available literature regarding abdominal aortic applications of CEUS, briefly elaborate on CEUS technique and safety and present cases in order to illustrate the added value in aortic pathologies. Conditions discussed include abdominal aortic aneurysm (AAA), aneurysm rupture, aneurysm surveillance after endovascular repair, dissection and aortitis.
Keywords: Aneurysm; aorta; aortitis; endoleak; ultrasonography.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Contrast-enhanced ultrasound of the abdominal aorta - current status and future perspectives.Vasa. 2019 Mar;48(2):115-125. doi: 10.1024/0301-1526/a000749. Epub 2018 Oct 16. Vasa. 2019. PMID: 30324867
-
Contrast Enhanced Ultrasound can Replace Computed Tomography Angiography for Surveillance After Endovascular Aortic Aneurysm Repair.Eur J Vasc Endovasc Surg. 2016 Dec;52(6):729-734. doi: 10.1016/j.ejvs.2016.07.007. Epub 2016 Oct 17. Eur J Vasc Endovasc Surg. 2016. PMID: 27760698
-
Prospective, single UK centre, comparative study of the predictive values of contrast-enhanced ultrasound compared to time-resolved CT angiography in the detection and characterisation of endoleaks in high-risk patients undergoing endovascular aneurysm repair surveillance: a protocol.BMJ Open. 2018 Apr 3;8(4):e020835. doi: 10.1136/bmjopen-2017-020835. BMJ Open. 2018. PMID: 29615450 Free PMC article.
-
Contrast-enhanced ultrasound (CEUS) of the abdominal vasculature.Abdom Radiol (NY). 2018 Apr;43(4):934-947. doi: 10.1007/s00261-017-1329-7. Abdom Radiol (NY). 2018. PMID: 28983674 Free PMC article. Review.
-
Contrast-enhanced ultrasound: clinical applications in patients with atherosclerosis.Int J Cardiovasc Imaging. 2016 Jan;32(1):35-48. doi: 10.1007/s10554-015-0713-z. Epub 2015 Jul 24. Int J Cardiovasc Imaging. 2016. PMID: 26206524 Free PMC article. Review.
Cited by
-
General principles and overview of vascular contrast-enhanced ultrasonography.Ultrasonography. 2020 Jan;39(1):22-42. doi: 10.14366/usg.19022. Epub 2019 Jun 25. Ultrasonography. 2020. PMID: 31671927 Free PMC article.
-
Reference for Normal Diameters of the Abdominal Aorta and Common Iliac Arteries in the Saudi Population.Cureus. 2022 Oct 26;14(10):e30695. doi: 10.7759/cureus.30695. eCollection 2022 Oct. Cureus. 2022. PMID: 36439581 Free PMC article.
-
Imaging Modalities for the Diagnosis of Vascular Graft Infections: A Consensus Paper amongst Different Specialists.J Clin Med. 2020 May 17;9(5):1510. doi: 10.3390/jcm9051510. J Clin Med. 2020. PMID: 32429584 Free PMC article. Review.
-
A novel approach for treating type II endoleaks utilizing contrast-enhanced ultrasound.J Vasc Surg Cases Innov Tech. 2021 Jun 12;7(3):581-585. doi: 10.1016/j.jvscit.2021.05.018. eCollection 2021 Sep. J Vasc Surg Cases Innov Tech. 2021. PMID: 34504986 Free PMC article.
-
Diagnostic Value of Contrast-Enhanced Ultrasound for Evaluation of Transjugular Intrahepatic Portosystemic Shunt Perfusion.Diagnostics (Basel). 2021 Sep 1;11(9):1593. doi: 10.3390/diagnostics11091593. Diagnostics (Basel). 2021. PMID: 34573935 Free PMC article.
References
-
- Claudon M, Dietrich CF, Choi BI, et al. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver--update 2012: a WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB, AIUM, ASUM, FLAUS and ICUS. Ultraschall Med 2013;34:11-29. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources