

Advanced endografting techniques: snorkels, chimneys, periscopes, fenestrations, and branched endografts
- PMID: 29850429
- PMCID: PMC5949586
- DOI: 10.21037/cdt.2017.08.17
Advanced endografting techniques: snorkels, chimneys, periscopes, fenestrations, and branched endografts
Abstract
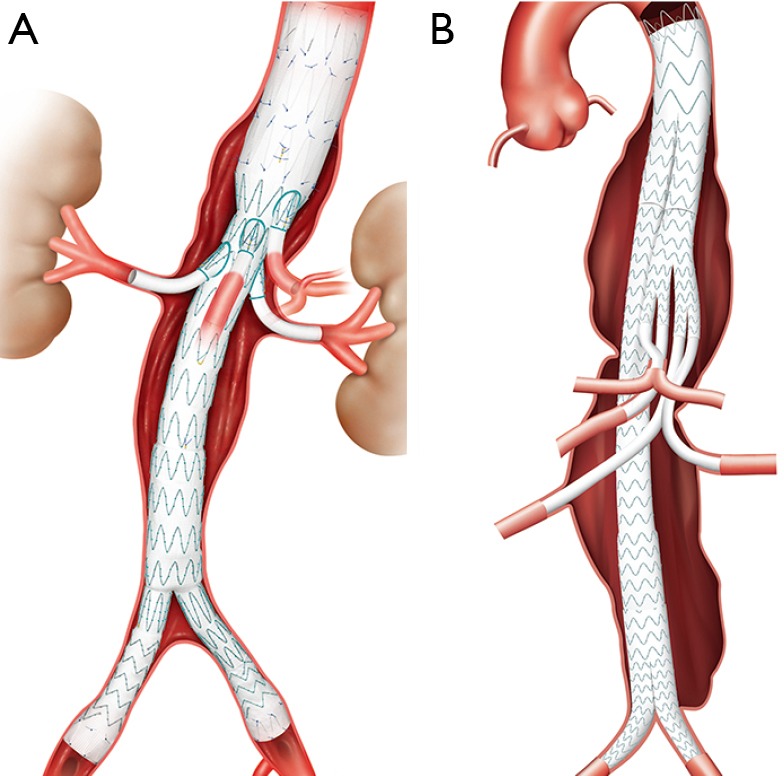
The anatomy of aortic aneurysms from the proximal neck to the access vessels may create technical challenges for endovascular repair. Upwards of 30% of patients with abdominal aortic aneurysms (AAA) have unsuitable proximal neck morphology for endovascular repair. Anatomies considered unsuitable for conventional infrarenal stent grafting include short or absent necks, angulated necks, conical necks, or large necks exceeding size availability for current stent grafts. A number of advanced endovascular techniques and devices have been developed to circumvent these challenges, each with unique advantages and disadvantages. These include snorkeling procedures such as chimneys, periscopes, and sandwich techniques; "homemade" or "back-table" fenestrated endografts as well as manufactured, customized fenestrated endografts; and more recently, physician modified branched devices. Furthermore, new devices in the pipeline under investigation, such as "off-the-shelf" fenestrated stent grafts, branched stent grafts, lower profile devices, and novel sealing designs, have the potential of solving many of the aforementioned problems. The treatment of aortic aneurysms continues to evolve, further expanding the population of patients that can be treated with an endovascular approach. As the technology grows so do the number of challenging aortic anatomies that endovascular specialists take on, further pushing the envelope in the arena of aortic repair.
Keywords: Abdominal aortic aneurysm (AAA); branched endograft; endovascular; fenestrated; snorkel.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials