

Practice Guideline
doi: 10.1093/eurheartj/ehy077.
International Expert Consensus Document on Takotsubo Syndrome (Part II): Diagnostic Workup, Outcome, and Management
Affiliations
- PMID: 29850820
- PMCID: PMC5991205
- DOI: 10.1093/eurheartj/ehy077
Item in Clipboard
Practice Guideline
International Expert Consensus Document on Takotsubo Syndrome (Part II): Diagnostic Workup, Outcome, and Management
Eur Heart J.
.
Abstract
The clinical expert consensus statement on takotsubo syndrome (TTS) part II focuses on the diagnostic workup, outcome, and management. The recommendations are based on interpretation of the limited clinical trial data currently available and experience of international TTS experts. It summarizes the diagnostic approach, which may facilitate correct and timely diagnosis. Furthermore, the document covers areas where controversies still exist in risk stratification and management of TTS. Based on available data the document provides recommendations on optimal care of such patients for practising physicians.
Figures
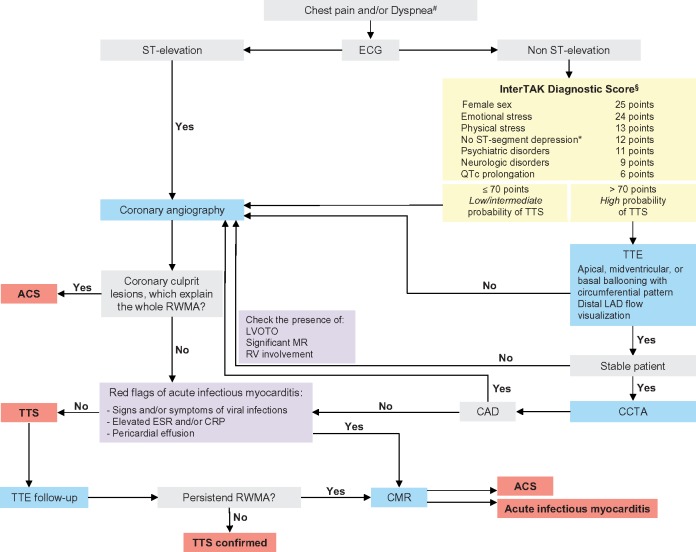
Diagnostic algorithm of takotsubo syndrome. #Applied to patients who are seeking medical emergency departments with e.g. chest pain and/or dyspnoea. §The InterTAK Diagnostic Score did not include patients with pheochromocytoma induced takotsubo syndrome in which atypical pattern are more frequently noted. *Except in lead aVR. ACS, acute coronary syndrome; CAD, coronary artery disease; CCTA, coronary computed tomography angiography; CMR, cardiac magnetic resonance; CRP, c-reactive protein; ECG, electrocardiogram; ESR, erythrocyte sedimentation rate; InterTAK, International Takotsubo Registry; LAD, left anterior descending coronary artery; LVOTO, left ventricular outflow tract obstruction; MR, mitral regurgitation; QTc, QT-time corrected for heart rate; RV, right ventricle; RWMA, regional wall motion abnormality; TTE, transthoracic echocardiography; TTS, takotsubo syndrome.
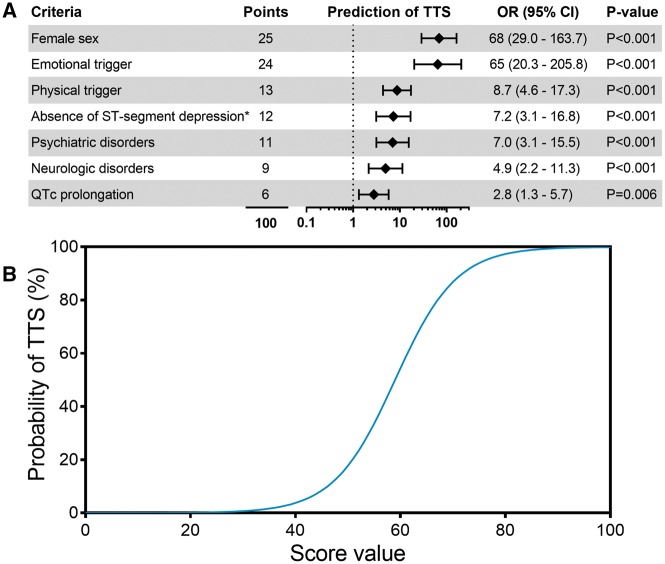
InterTAK Diagnostic Score. Predictors for diagnosing takotsubo syndrome by multiple logistic regression analysis. Odds ratios of the parameters female sex, emotional trigger, physical trigger, absence of ST-segment depression, psychiatric disorders, neurologic disorders, and QTc prolongation, which were chosen to build the InterTAK Diagnostic Score. *Except in lead aVR (A). Sigmoid curve shows the estimated prevalence of takotsubo syndrome in clinical practice (B). Modified and reprinted with permission from Ghadri et al.. CI, confidence interval; OR, odds ratio; QTc, QT-time corrected for heart rate; TTS, takotsubo syndrome.
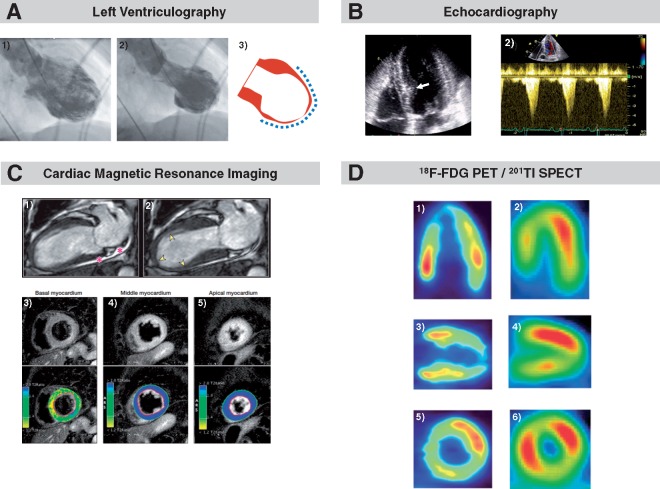
Apical ballooning illustrated by different imaging modalities. Typical takotsubo type with apical ballooning pattern during diastole (A.1) and systole (A.2) on left ventriculography. Dashed lines indicate extent of wall motion abnormality (A.3). Modified and reprinted with permission from Templin et al. Apical four-chamber view obtained by echocardiography showing apical ballooning and left ventricular cavity with bulging of the basal interventricular septum (white arrow) (B.1). B.2 reveals left ventricular outflow tract obstruction by pulsed-wave Doppler interrogation. Modified and reprinted with permission from Merli et al. Apical ballooning as illustrated by cardiac magnetic resonance imaging. The asterisks indicate pericardial effusion (C.1) and yellow arrows (C.2) shows the region of akinesia. T2-weighted images on short-axis view demonstrates normal signal intensity of the basal myocardium (C.3) and global oedema of the mid and apical myocardium (C.4 and C.5). Modified and reprinted with permission from Eitel et al. Metabolic imaging with positron emission tomography and 18F-flurodeoxyglucose (D.1, D.3, D.5) demonstrates decreased uptake in the apex and midventricular segments. Perfusion imaging using single photon emission computed tomography with 201thallium chloride (D.2, D.4, D.6) shows a smaller perfusion defect in the apex and midventricular segments. Reprinted with permission from Yoshida et al.
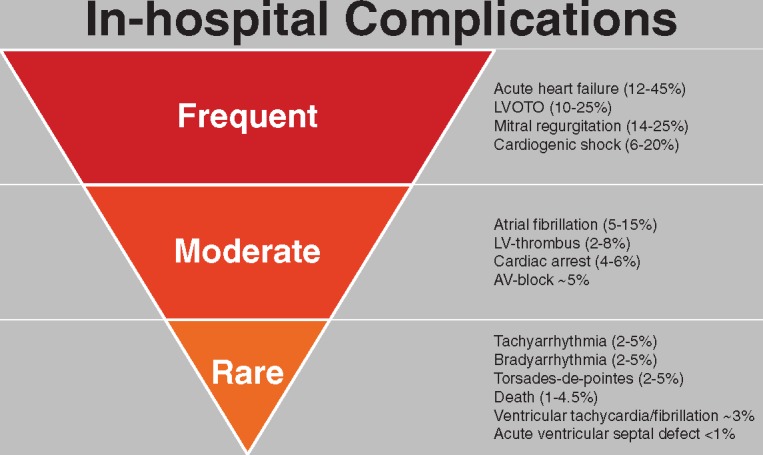
Overview of in-hospital complications according to their prevalence. AV, atrioventricular block; LV, left ventricle; LVOTO, left ventricular outflow tract obstruction.
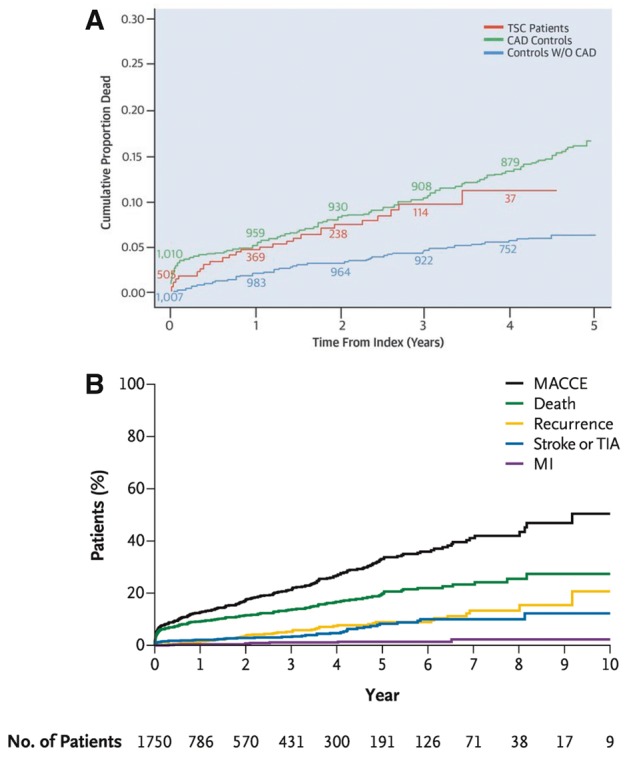
Long-term outcome (5-years) of patients with TTS compared to patients with and without CAD (A). Long-term outcome (10-years) of patients with TTS (B). MACCE refers to a composite of death from any cause, recurrence of takotsubo syndrome, stroke or transient ischaemic attack, or myocardial infarction. CAD, coronary artery disease; MACCE, major adverse cardiac and cerebrovascular event; MI, myocardial infarction; TIA, transient ischaemic attack; TSC, takotsubo stress cardiomyopathy. Reprinted with permission from Tornvall et al. and Templin et al.
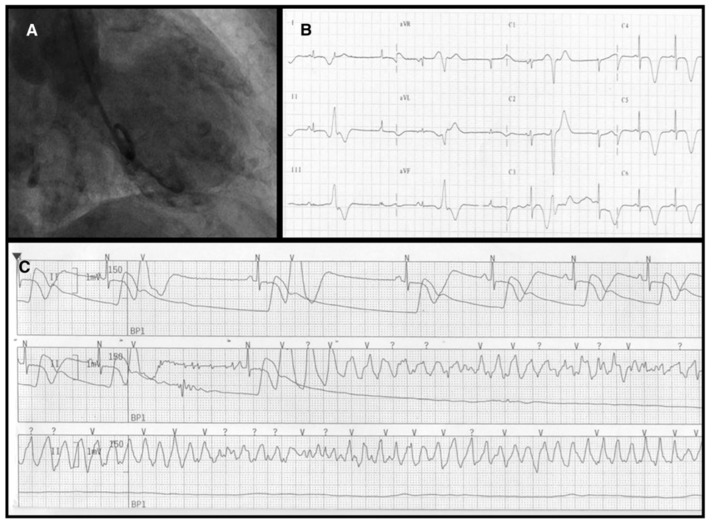
Arrhythmic complication in takotsubo syndrome. Left ventriculography (antero-posterior view) showing the typical apical ballooning pattern with akinesia of the mid-apical segments and hyperkinesia of the basal segment (A). A 12-lead electrocardiogram recorded at the third day of hospitalization showing giant negative T-waves in leads aVL, L1, L2, aVF and V4–V6, marked QT prolongation (QTc = 552 ms) and ‘R on T’ premature ventricular beats (B). Telemetry recording of a pause-dependent (‘long-short sequence’) torsade-de-pointes/ventricular fibrillation, which required electrical cardioversion (C). Reprinted with permission from Migliore et al.
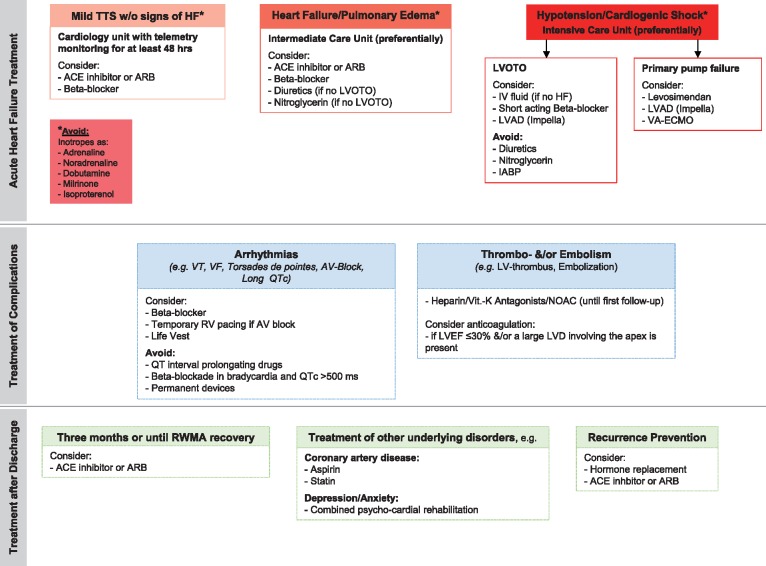
Management of takotsubo syndrome. ACE, angiotensin-converting-enzyme; ARB, angiotensin-receptor blocker; AV-block, atrioventricular block; HF, heart failure; IABP, intra-aortic balloon pump; IV, intravenous; LV, left ventricle; LVAD, left ventricular assist device; LVD, left ventricular dysfunction; LVEF, left ventricular ejection fraction; LVOTO, left ventricular outflow tract obstruction; NOAC, novel oral anticoagulant; QTc, QT-time corrected for heart rate; RV, right ventricle; TTS, takotsubo syndrome; VA-ECMO, venoarterial extracorporeal membrane oxygenation; VF, ventricular fibrillation; VT, ventricular tachycardia.
References
-
- Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E.. Apical ballooning syndrome or Takotsubo cardiomyopathy: a systematic review. Eur Heart J 2006;27:1523–1529. - PubMed
-
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, Cammann VL, Sarcon A, Geyer V, Neumann CA, Seifert B, Hellermann J, Schwyzer M, Eisenhardt K, Jenewein J, Franke J, Katus HA, Burgdorf C, Schunkert H, Moeller C, Thiele H, Bauersachs J, Tschöpe C, Schultheiss H-P, Laney CA, Rajan L, Michels G, Pfister R, Ukena C, Böhm M, Erbel R, Cuneo A, Kuck K-H, Jacobshagen C, Hasenfuss G, Karakas M, Koenig W, Rottbauer W, Said SM, Braun-Dullaeus RC, Cuculi F, Banning A, Fischer TA, Vasankari T, Airaksinen KEJ, Fijalkowski M, Rynkiewicz A, Pawlak M, Opolski G, Dworakowski R, MacCarthy P, Kaiser C, Osswald S, Galiuto L, Crea F, Dichtl W, Franz WM, Empen K, Felix SB, Delmas C, Lairez O, Erne P, Bax JJ, Ford I, Ruschitzka F, Prasad A, Lüscher TF.. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N Engl J Med 2015;373:929–938. - PubMed
-
- Prasad A, Lerman A, Rihal CS.. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J 2008;155:408–417. - PubMed
-
- Bennett J, Ferdinande B, Kayaert P, Wiyono S, Goetschalkx K, Dubois C, Sinnaeve P, Adriaenssens T, Coosemans M, Desmet W.. Time course of electrocardiographic changes in transient left ventricular ballooning syndrome. Int J Cardiol 2013;169:276–280. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
