

The Applicability of a High-Intensity Functional Exercise Program Among Older People With Dementia Living in Nursing Homes
- PMID: 29851748
- PMCID: PMC6791515
- DOI: 10.1519/JPT.0000000000000199
The Applicability of a High-Intensity Functional Exercise Program Among Older People With Dementia Living in Nursing Homes
Abstract
Background and purpose: Exercise programs for people with dementia need to be optimized. We therefore evaluated the applicability of a high-intensity functional exercise program among people with dementia in nursing homes with regard to attendance, achieved exercise intensity, adverse events, a focus on dementia type, and whether symptoms of dementia or other medical conditions common in this population were associated with program applicability.
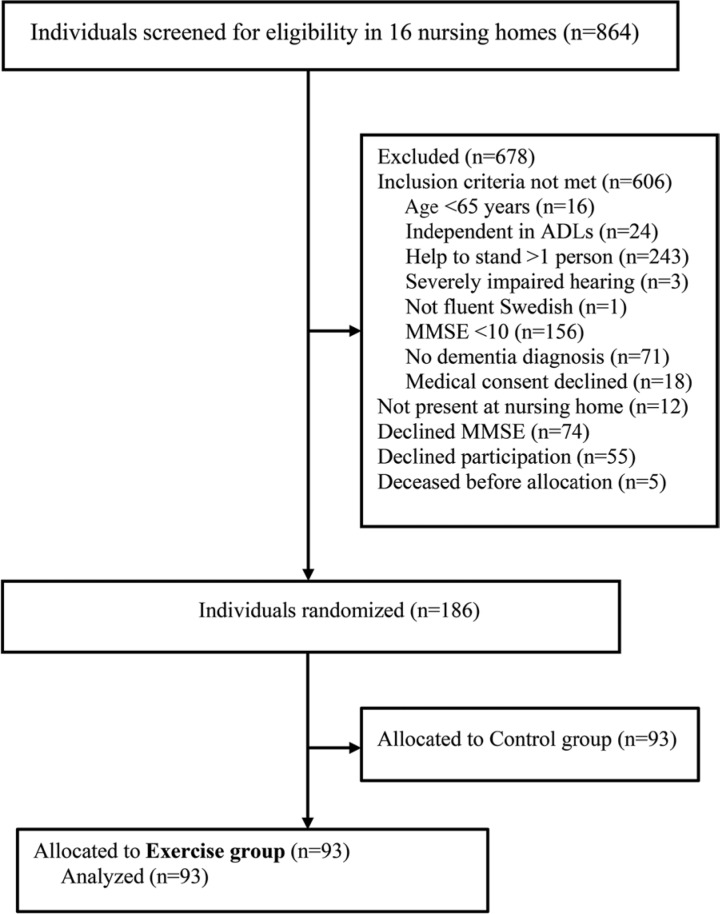
Methods: The Umeå Dementia and Exercise study, a cluster-randomized controlled trial set in 16 nursing homes in Umeå, Sweden. Ninety-three people with dementia (mean [SD] Mini-Mental State Examination score of 15.4 [3.4]) were randomized to the exercise intervention. Thirty-four participants had Alzheimer's disease (AD) and 59 non-Alzheimer's dementia (non-AD). High-Intensity Functional Exercise (HIFE) program was conducted in groups of 3 to 8 participants. Two physiotherapists led 5 sessions (45 minutes each) per fortnight for 4 months (total 40 sessions).
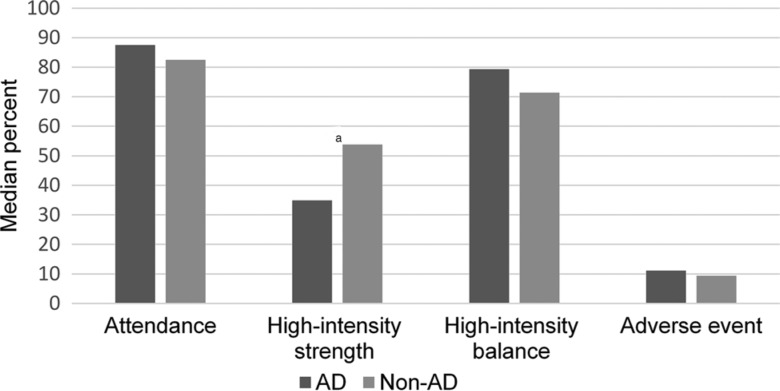
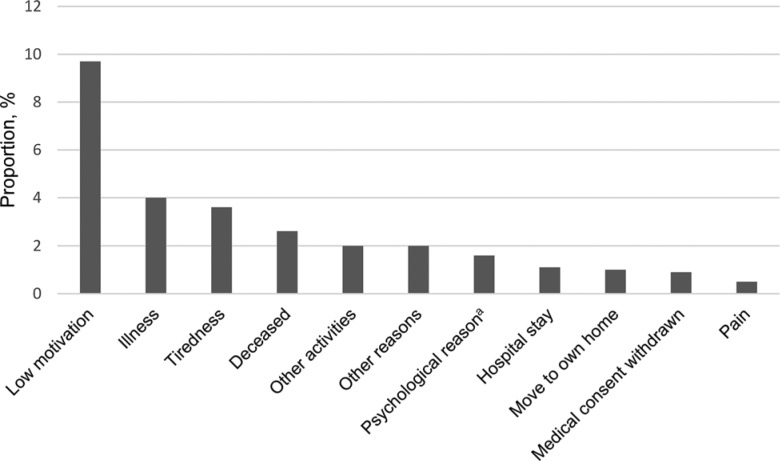
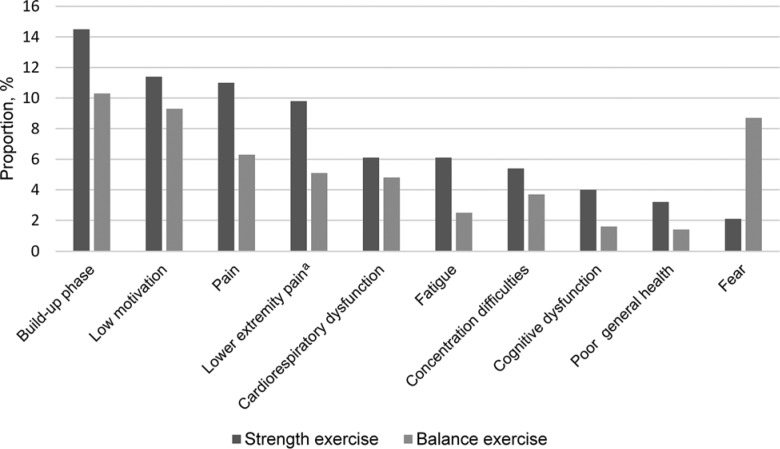
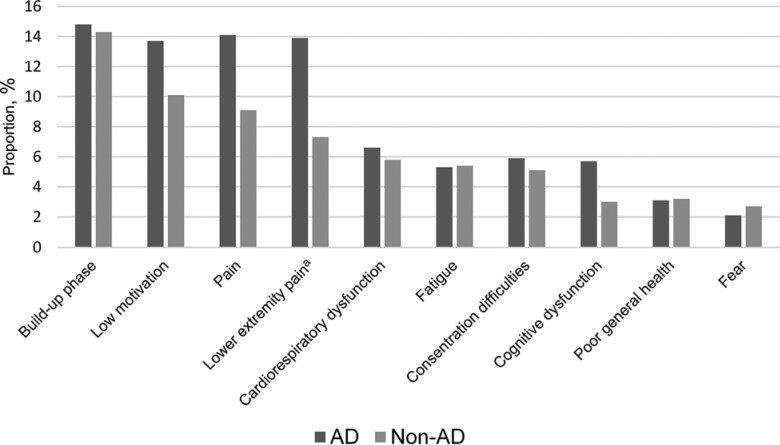
Results: Median attendance rate was 82.5%. Lower limb strength exercises were performed at high or medium intensity at a median interquartile range of 94.7% (77.8%-100%) of attended sessions. Participants with non-AD performed more sessions with high intensity in strength exercises than participants with AD (median interquartile range, 53.8% [25.7%-80%] vs 34.9% [2.02%-62.9%]; P = .035). Balance exercises were performed at high intensity at a median interquartile range of 75% (33.3%-88.6%). Adverse events (all minor and temporary, mostly musculoskeletal) occurred during the exercise sessions in 16% of attended sessions. Low motivation was the most common barrier for attendance. Buildup period, low motivation, and pain were common barriers for achieving high intensity in balance and strength exercises, and fear was a barrier in balance exercises. Of medical conditions, only behavioral and psychological symptoms of dementia, including apathy, were negatively associated with applicability.
Conclusion: A group-based, supervised, and individualized high-intensity functional exercise program seems to be applicable with regard to attendance, achieved intensity, and adverse events during the exercise sessions, in people with mild to moderate dementia in nursing homes. Effective strategies to enhance motivation to participate in exercise, as well as prevention and treatment of pain and behavioral and psychological symptoms of dementia, are important when promoting exercise participation in this population.
Conflict of interest statement
H.L. and N.L. developed and have received royalties on the weighted belt used in the exercise program. All other authors declare no conflicts of interest.
Figures
References
-
- World Health Organization. Dementia: a public health priority. http://www.who.int/mental_health/publications/dementia_report_2012/en/. Published 2012. Accessed December 14, 2014.
-
- Sherrington C, Michaleff ZA, Fairhall N, et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med. 2017;51(24):1750–1758. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
