

Improved Brain Penetration and Antitumor Efficacy of Temozolomide by Inhibition of ABCB1 and ABCG2
- PMID: 29852323
- PMCID: PMC6030392
- DOI: 10.1016/j.neo.2018.05.001
Improved Brain Penetration and Antitumor Efficacy of Temozolomide by Inhibition of ABCB1 and ABCG2
Abstract
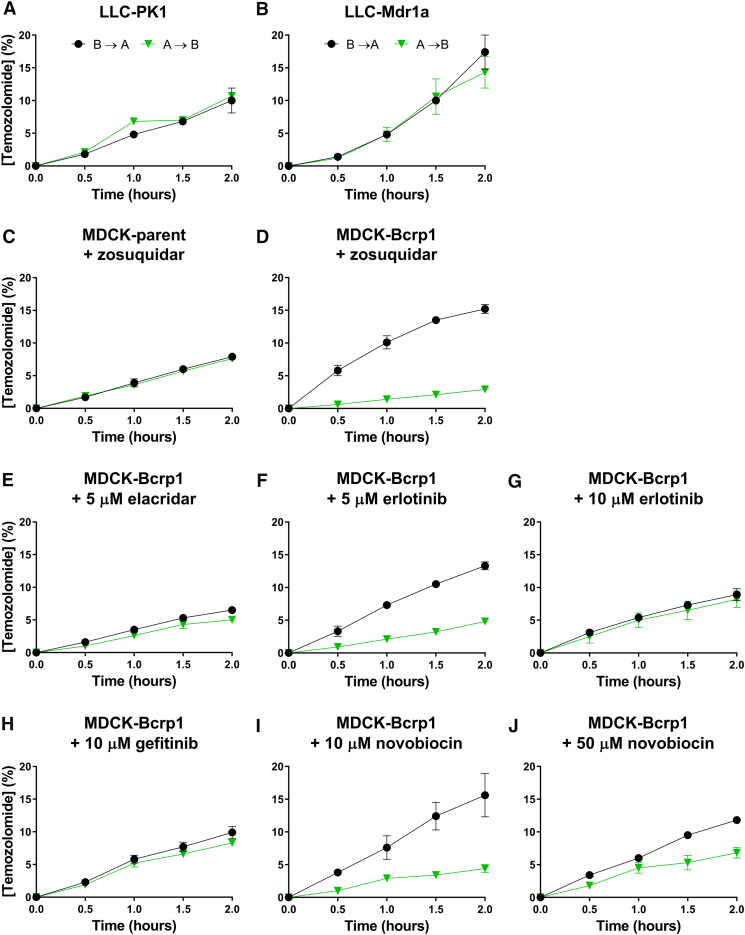
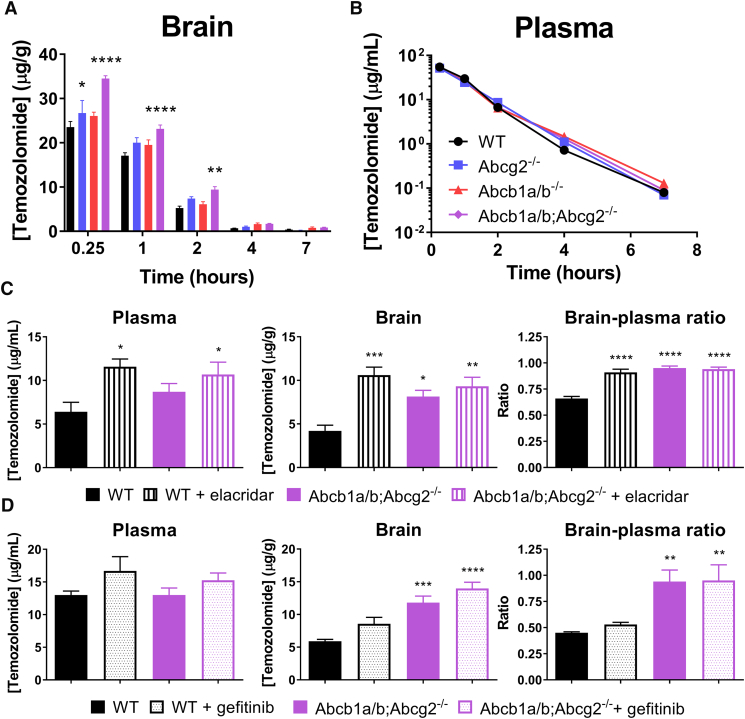
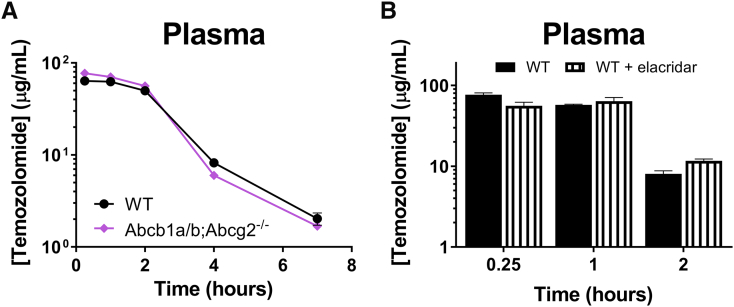
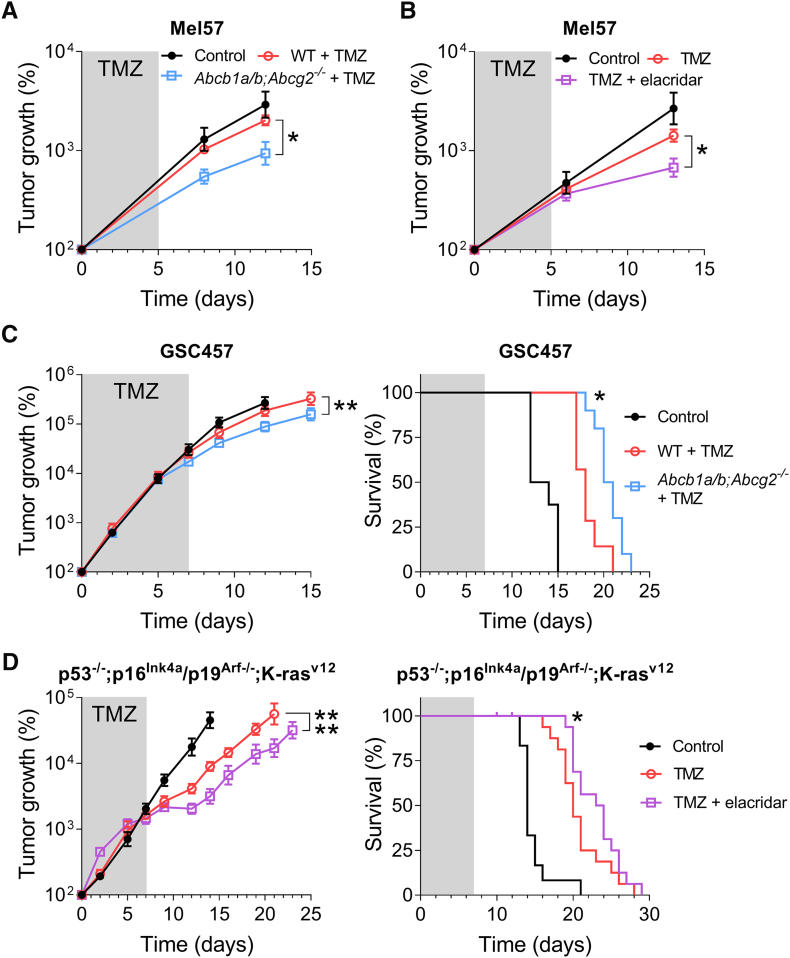
The anticancer drug temozolomide is the only drug with proven activity against high-grade gliomas and has therefore become a part of the standard treatment of these tumors. P-glycoprotein (P-gp; ABCB1) and breast cancer resistance protein (BCRP; ABCG2) are transport proteins, which are present at the blood-brain barrier and limit the brain uptake of substrate drugs. We have studied the effect of P-gp and BCRP on the pharmacokinetics and pharmacodynamics of temozolomide, making use of a comprehensive set of in vitro transport experiments and in vivo pharmacokinetic and antitumor efficacy experiments using wild-type, Abcg2-/-, Abcb1a/b-/-, and Abcb1a/b;Abcg2-/- mice. We here show that the combined deletion of Abcb1a/b and Abcg2 increases the brain penetration of temozolomide by 1.5-fold compared to wild-type controls (P < .001) without changing the systemic drug exposure. Moreover, the same increase was achieved when temozolomide was given to wild-type mice in combination with the dual P-gp/BCRP inhibitor elacridar (GF120918). The antitumor efficacy of temozolomide against three different intracranial tumor models was significantly enhanced when Abcb1a/b and Abcg2 were genetically deficient or pharmacologically inhibited in recipient mice. These findings call for further clinical testing of temozolomide in combination with elacridar for the treatment of gliomas, as this offers the perspective of further improving the antitumor efficacy of this already active agent.
Copyright © 2018. Published by Elsevier Inc.
Figures
References
-
- van Tellingen O, Yetkin-Arik B, de Gooijer MC, Wesseling P, Wurdinger T, de Vries HE. Overcoming the blood-brain tumor barrier for effective glioblastoma treatment. Drug Resist Updat. 2015;19:1–12. - PubMed
-
- Pencheva N, de Gooijer MC, Vis DJ, Wessels LFA, Würdinger T, van Tellingen O, Bernards R. Identification of a druggable pathway controlling glioblastoma invasiveness. Cell Rep. 2017;20(1):48–60. - PubMed
-
- Abbott NJ, Patabendige AA, Dolman DE, Yusof SR, Begley DJ. Structure and function of the blood-brain barrier. Neurobiol Dis. 2010;37(1):13–25. - PubMed
-
- Durmus S, Hendrikx JJMA, Schinkel AH. Apical ABC transporters and cancer chemotherapeutic drug disposition. Adv Cancer Res. 2015;125:1–41. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
