

Review
doi: 10.2174/1573405613666170403102235.
Craniocervical Dissections: Radiologic Findings, Pitfalls, Mimicking Diseases: A Pictorial Review
Affiliations
- PMID: 29853818
- PMCID: PMC5902863
- DOI: 10.2174/1573405613666170403102235
Item in Clipboard
Review
Craniocervical Dissections: Radiologic Findings, Pitfalls, Mimicking Diseases: A Pictorial Review
Curr Med Imaging Rev.
2018 Apr.
Abstract
Background: Craniocervical Dissections (CCD) are a crucial emergency state causing 20% of strokes in patients under the age of 45. Although DSA (digital substraction angiography) is regarded as the gold standard, noninvasive methods of CT, CTA and MRI, MRA are widely used for diagnosis.
Aim: Our aim is to illustrate noninvasive imaging findings in CCD.
Conclusion: Emphasizing on diagnostic pitfalls, limitations and mimicking diseases.
Keywords: CT; CTA; Craniocervical dissection; DSA; MRA; MRI.
Figures
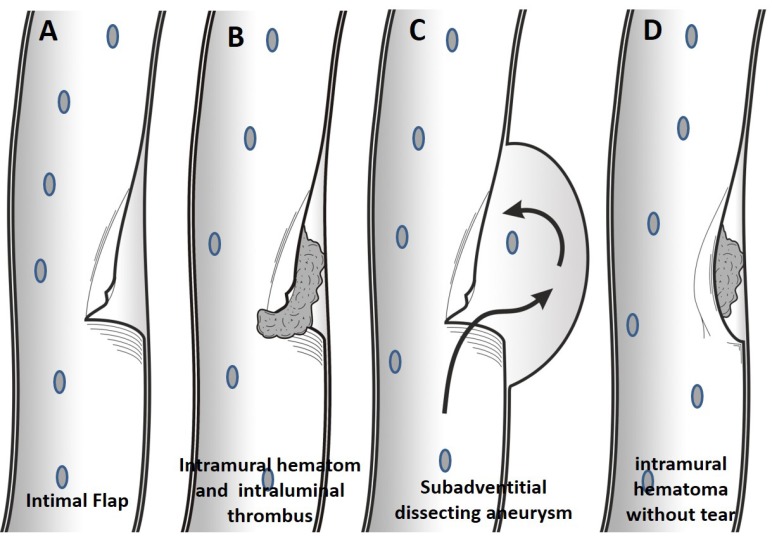
In dissection with intimal flap tear without thrombus formation, patient will be presenting only with pain (A). More extensive tear will result in intraluminal and subintimal thrombus formation, therefore, thromboembolic event is more common in this group (B). In dissecting aneurysm, the wall tear will extend into subadventitial region, and the adventitia will be weakened and widened, resulting in the subadventitial aneurysm limited by the adventitia. (C). Without intimal tear, intramural thrombus may occur by leakage from vaso vasorum within media layer in arteriopathic patients (D).
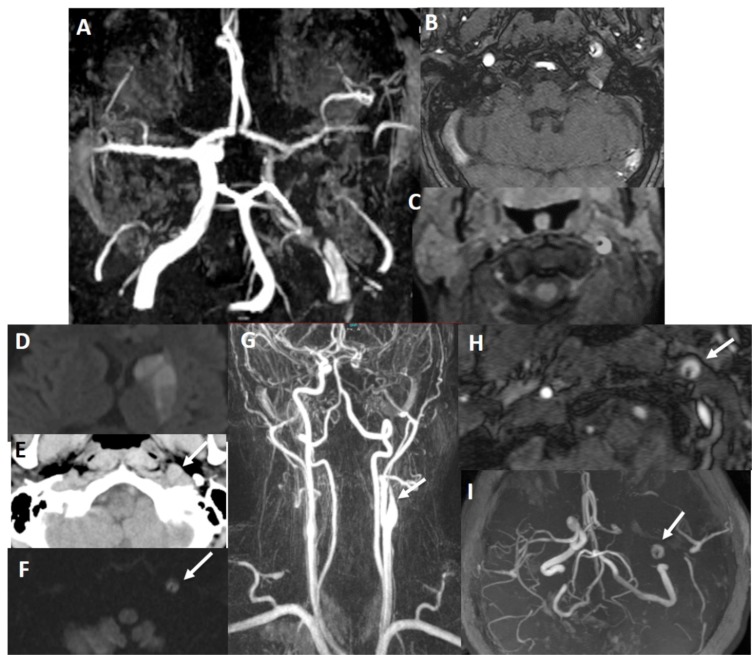
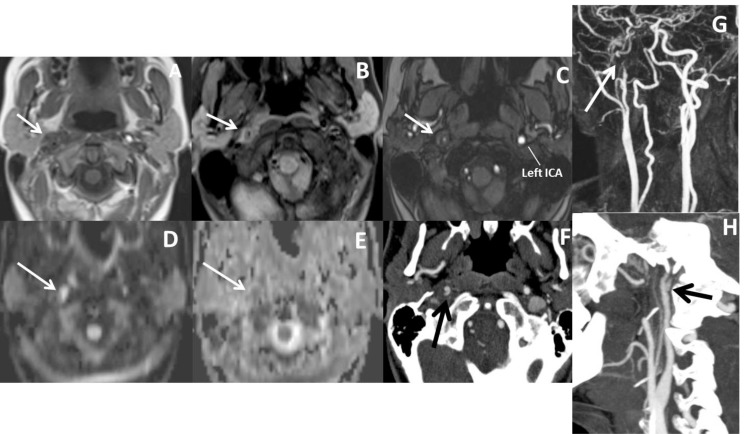
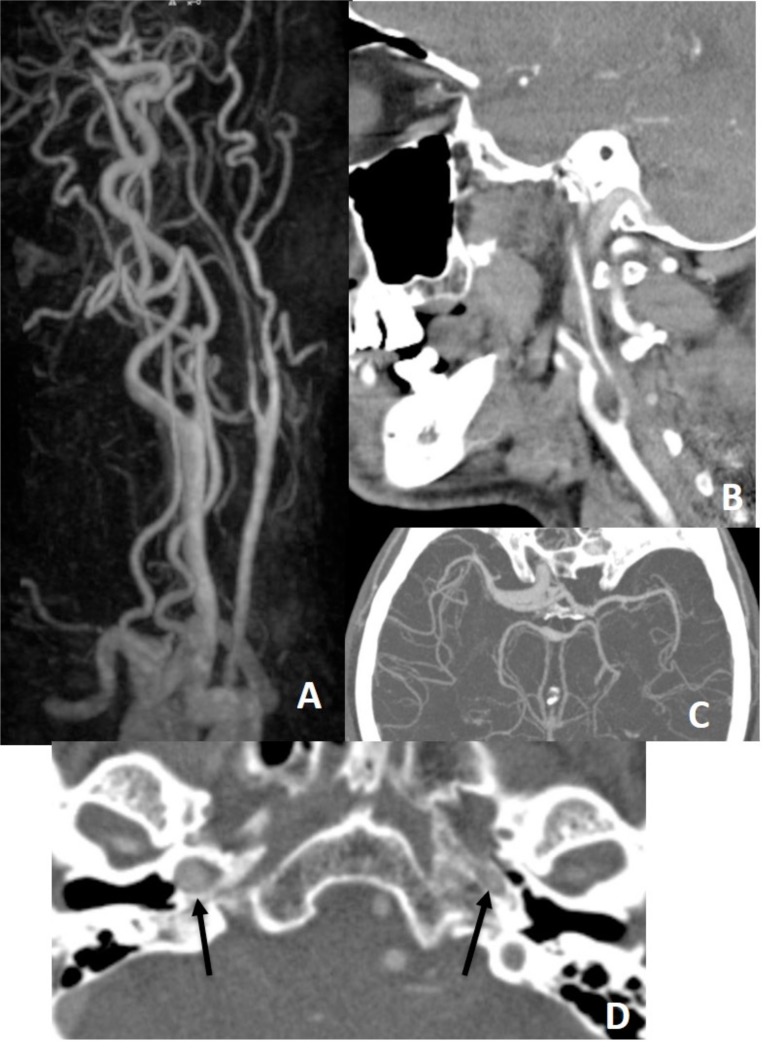
There is false double lumen appearance of left petrous ICA on MIP (A) and source (B) views of 3D TOF MRA. Fat suppressed T1 image show crescent sign of hyperintense intramural thrombus, increased external diameter of left ICA with eccentric luminal narrowing (C). Not: intramural thrombus is seen hyperintense on 3D TOF MRA, giving false appearance of double lumen. In another patient with left sided acute striatal stroke (D), arrows show left ICA as enlarged and hyperdense on CT (E) associated with diffusion signal changes on DWI (F). On contrast enhanced neck MRA, flame sign of left ICA is seen with very limited flow distally (arrow on G) and associated enlarged external diameter of left ICA with crescent sign and eccentric luminal narrowing appearing in both source (arrow on H) and MIP (arrow on I) images of 3D-TOF brain MRA. Findings are compatible with dissection of left ICA at the skull base where the enlargement of the vessel is present.
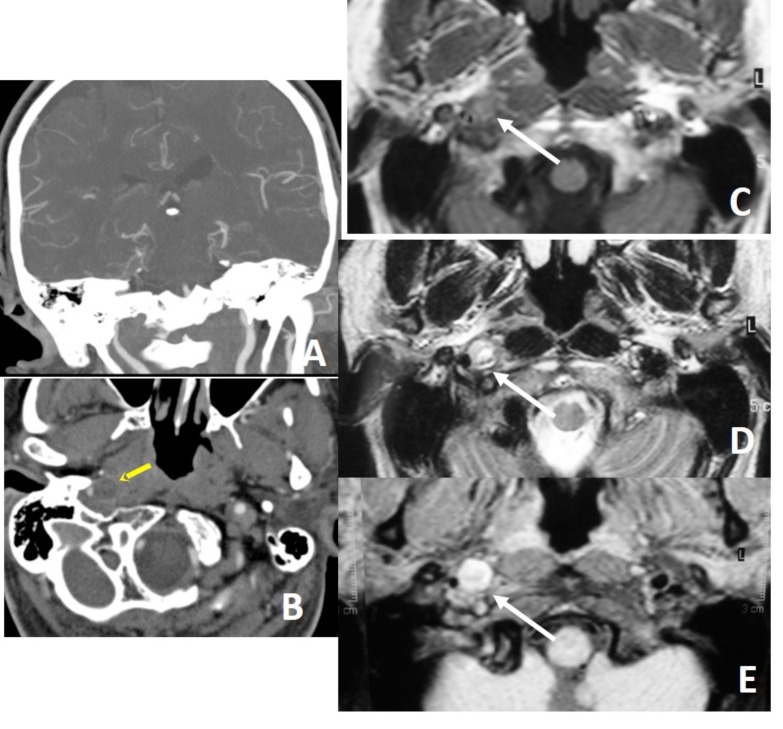
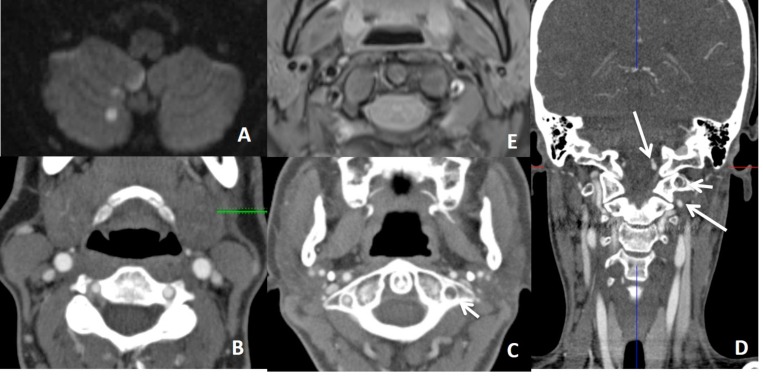
Distal cervical ICA is narrowed (A) with target sign (arrow on B) on CTA, compatible with dissection. Intramural thrombus is hard to see on T1W image (C), but hyperintense on T2W (D) and fat suppressed T1W (E) images (arrows), giving crescent sign on MRI. Thin annular enhancement of vessel wall with eccentric luminal narrowing gives target sign on CTA. Thin annular enhancement of vessel wall is due to the contrast enhancement of the adventitial layer via vaso vasorum.
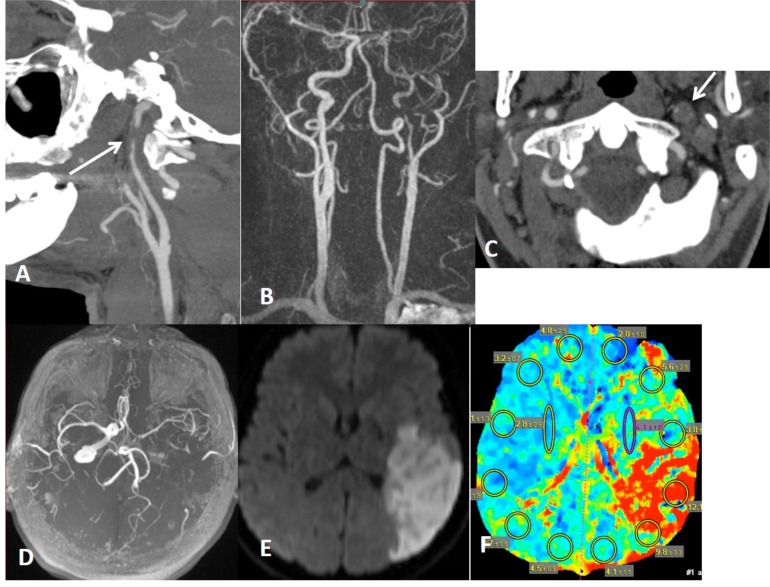
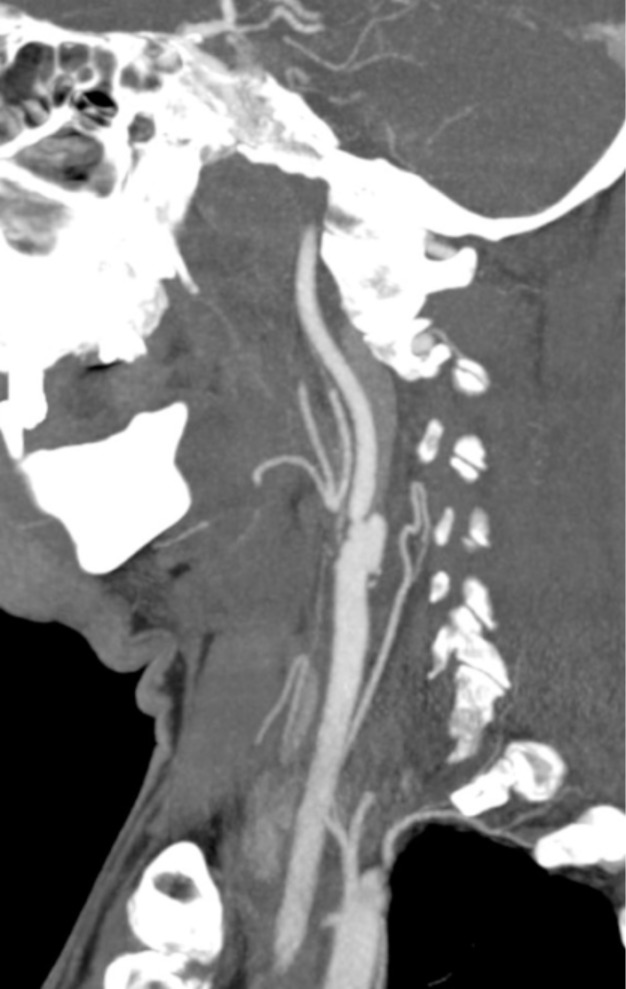
Left distal cervical ICA dissection with focal stenosis (string sign) on CTA (arrow on A) and MRA (B) with target sign on CTA (arrow on C). There is limitation flow in the left MCA territory on MRA (B and D) with hemodynamic infartcion on DWI (E) associated with penumbra on CT perfusion (F).
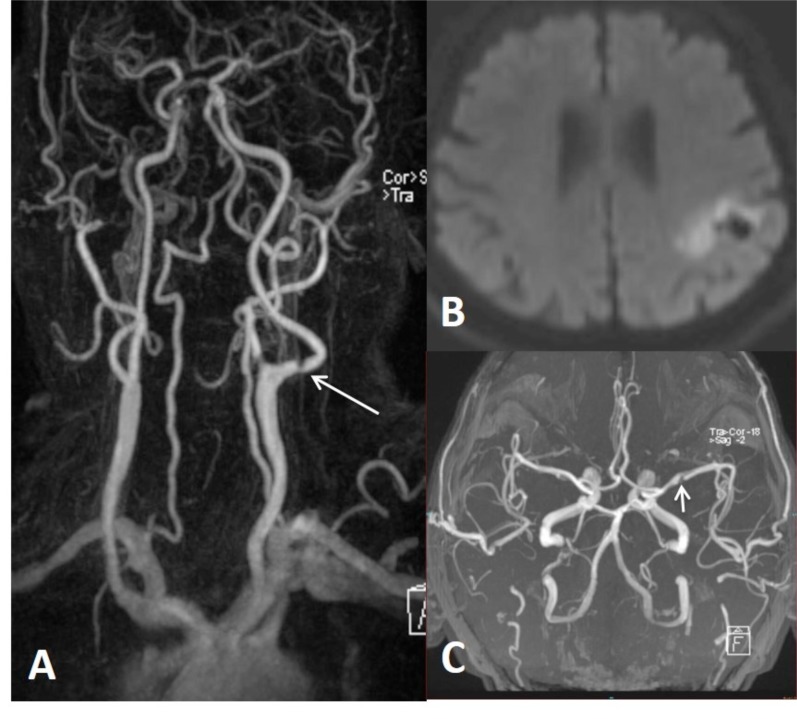
Intimal flap type dissection of left ICA on contrast enhanced MRA (arrow on A) distal to bulbus with thromboembolic infarction in left MCA territory on DWI (B). Intimal flap type dissection of left M1 on brain MRA (C) in another patient with a history of right sided paresis, difficulty in speaking, visual problem and tinnitus 11 days ago.
Contrast enhanced MRA show stenosis of distal cervical ICA (arrow on A). Axial T2W shows hypointense true lumen of right ICA surrounded by hyperintense pseudolumen (arrow on B). Hyperintensity is due to sluggish blood flow or thrombosis within pseudolumen.
In a patient with right sided visual loss there is focal narrowing of right ICA distal to bulbus (A) and increased external diameter and concentric mural thickening of right ICA comparing the left one (arrows on B), compatible with right ICA dissection. In this case, true lumen is not eccentric, almost centrally located. There is sluggish blood flow in the distal right ICA (C).
Dissecting aneurysm of left distal cervical ICA on MRA. Dissecting aneurysm is a finding of extracranial dissection, observed in 1/3 of extracranial dissections. Intracranial dissections mostly result in subarachnoid bleeding. Dissecting anurysm of basilar tip (arrow on B) in another patient results in extraaxial hematoma surrounding the dissected vessel (arrow on C) and diffuse subarachnoid bleeding (D).
In a patient with right sided Horner syndrome short white arrows show increase in external diameter of distal cervical ICA on axial T1 (A), hyperintensity in the wall of the vessel secondary to intramural thrombus on fat-sat axial T1A (B), eccentric luminal narrowing and mural thickening on source image of 3D- TOF MRA (C), diffusion changes related to blood product within the wall of the vessel on DWI (D) and corresponding ADC map (E), contrast extravasation from the narrowed lumen into thickened vessel wall on axial CTA (F), narrowed right ICA at the skull base on contrast enhanced MRA (G) and dissecting aneurysm on sagittal MIP of CTA (H).
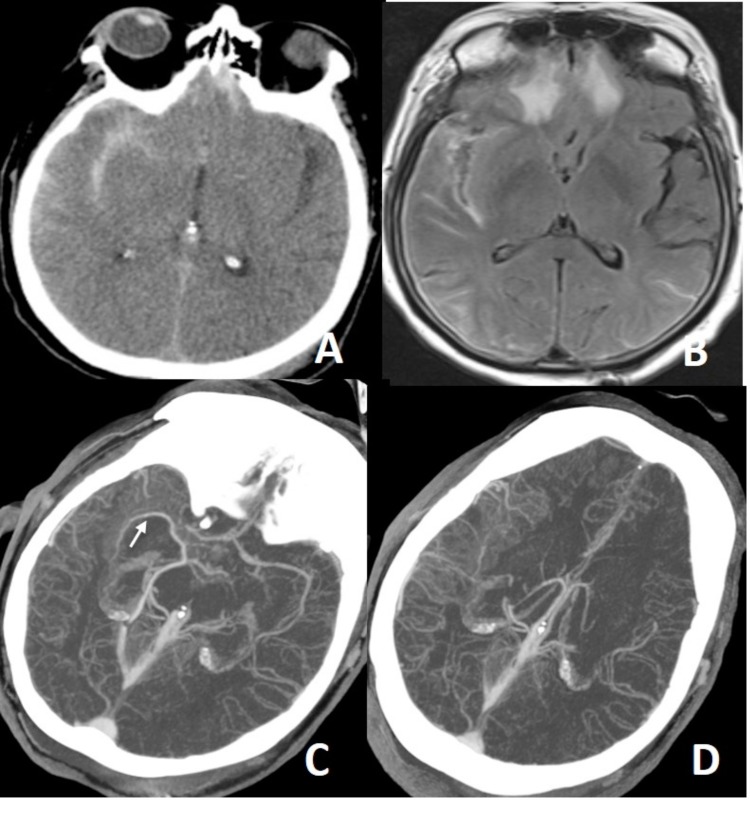
In a patient with a history of trauma, there is massive subarachnoid bleeding in right sylvian fissure (A) and parenchymal contusions in right temporal and frontal lobes (B). Axial MIP CTA images (C, D) show occlusion of right M1 segment and increased leptomeningeal-pial collateralization in the right MCA territory. Findings are compatible with postraumatic grade 5 dissection. Not: the arrow on C show middle cerebral vein spilling into the basal vein of Rosenthal.
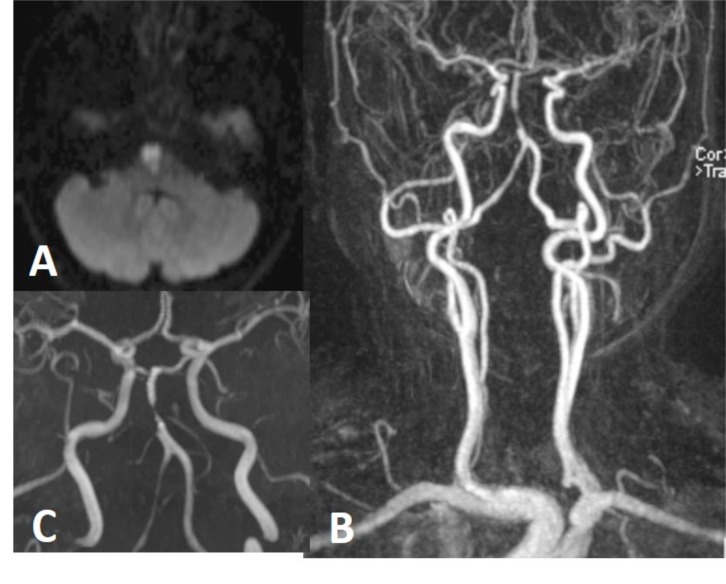
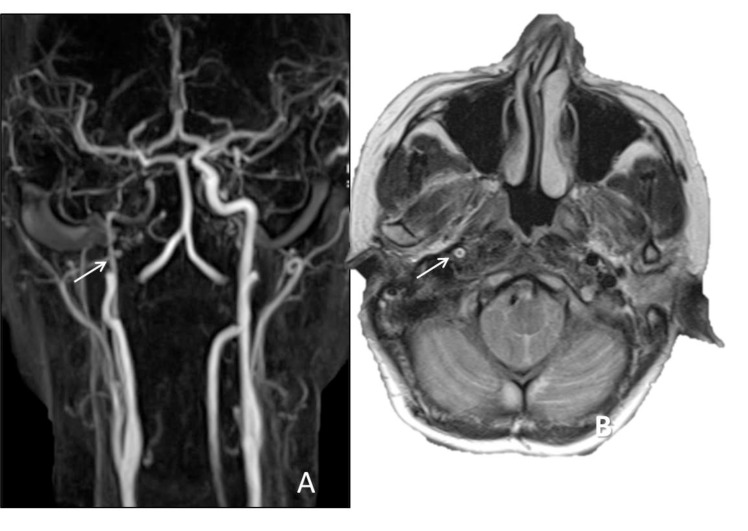
6 months earlier neck and brain MRA performed for tinnitus was normal (not shown here). Upon the presentation of brain stem acute infarction (A), neck (B) and brain (C) MRA were repeated showing focal narrowing (string sign), compatible with basilar artery dissection.
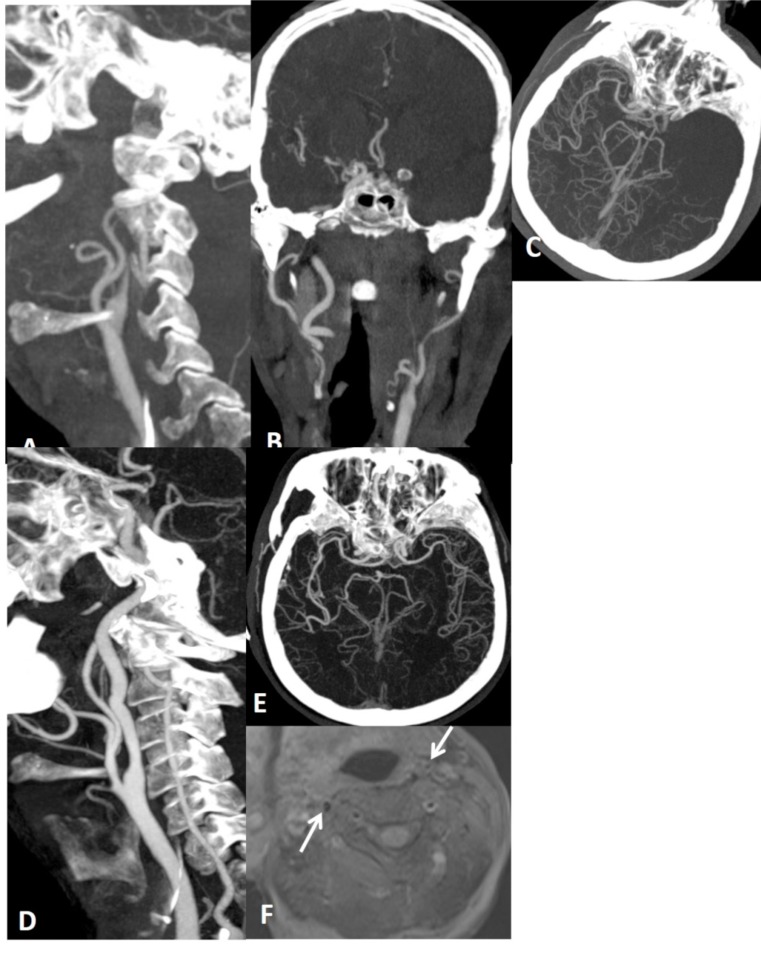
Axial Flair (A) and DWI (B) show different ages of thromboembolic infarctions in the brain stem and right cerebellum. Focal narrowing of right VA is seen on a MIP image of brain MRA (C). Source images of 3D TOF MRA from caudal to cranial (D-F) show eccentric luminal narrowing associated with increased external diameter of right VA due to intramural hematoma which is seen minimally hyperintense on E (arrow).

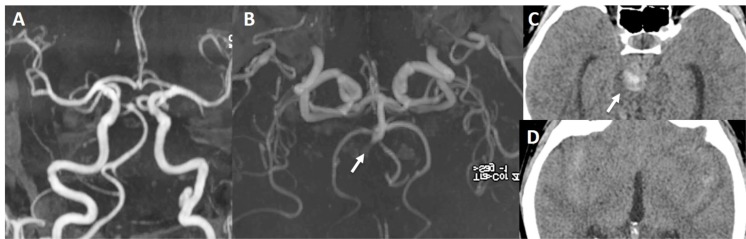
In a patient with recurrent thromboembolic infarction within the posterior circulation (A), brain MRA shows double lumen appearance of basiler artery. Flow is present in both lumen (B, C). Dissection is extending into right VA with hyperintense mural thickening (arrow on D), better seen in source image (D) than MIP image (E) of 3D TOF MRA.
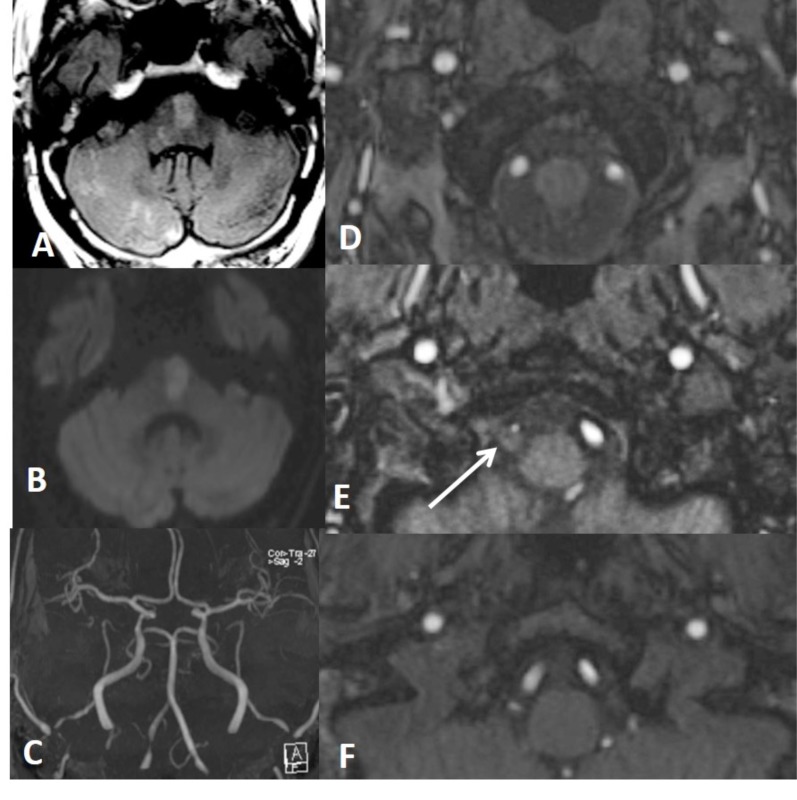
In a patient with thromboembolic infarction within right cerebellum (A), CTA (B, C, D) shows normal caliber of left VA at the proximal part of the V3 and V4 but narrowed at the distal part of the V3 (short arrow showing distal V3 on C) (long arrows showing proximal V3 and V4 on D). Distal V3 narrowing (C) is associated with intramural hematoma (crescent sign) on fat sat T1W images (E). Findings are suggestive of distal V3 dissection.
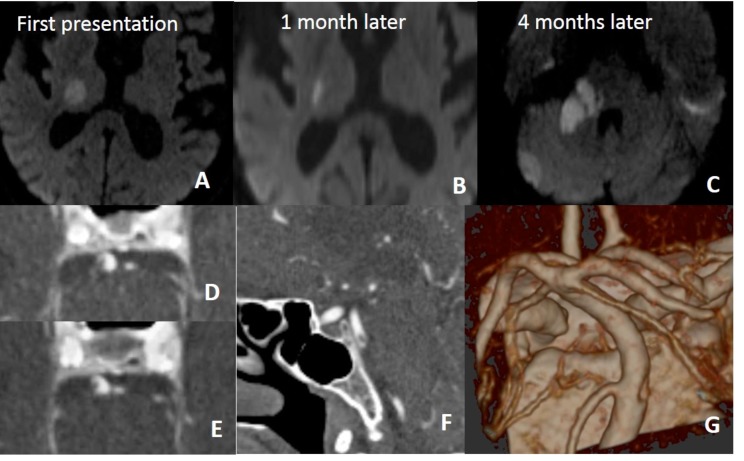
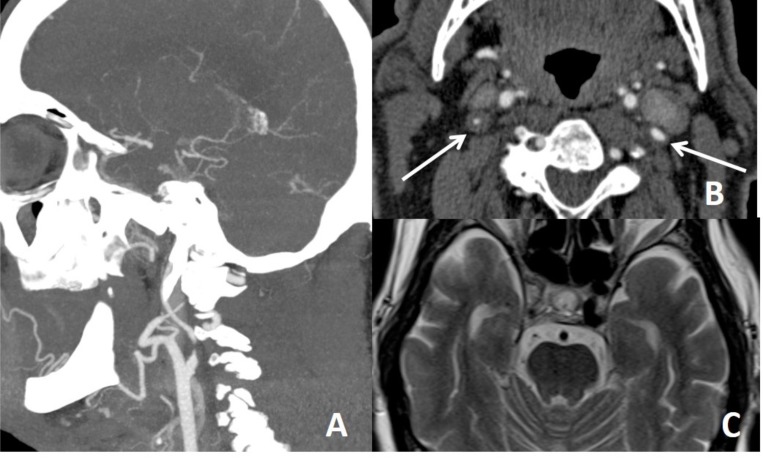
In a patient with recurrent infarction within the posterior circulation, brain and neck MRA (not shown here) repeated a few times were all normal. On 4th months, CTA was performed for vertebrobasiler system evaluation. There is dissection of intimal flap type tearing of basiler artery on CTA (D, E, F, G).
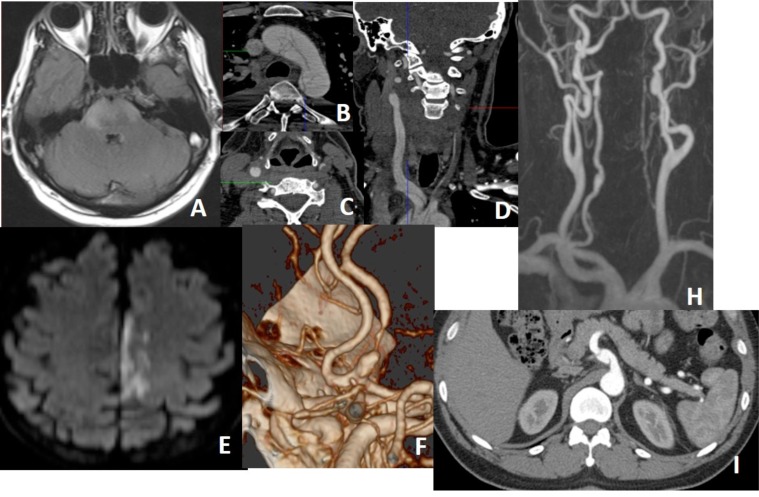
Vasculitis is big mimicker of dissection. On the other hand, vasculitis the one of causes of dissection. In a patient with Behcet’s disease, there is brain stem infarction (A) and intimal flap type dissection of arcus aorta (B) and bilateral CCAs (C, D) on CTA. All lumens in dissected arcus aorta is filling (B). Both two lumens in the right CCA is filling while filling lumen (true lumen) is very thin and other (false lumen) is is thrombosed in the left CCA (C, D). In another patient with osteogenesis imperfecta type 1, there is infarction within the left ACA territory (E) with focal narrowing and dialation (string and pearl sign) of left A2 on the volume rendering CTA (F), consisting with dissection of proximal part of left A2. In another patient with Behcet’s disease, vessel wall irregularities with saccular dilatations (pseudoaneurysms) are seen along the both ICAs and right VA (H). Pseudoaneurysm of the celiac trunk is seen in the same patient (I).
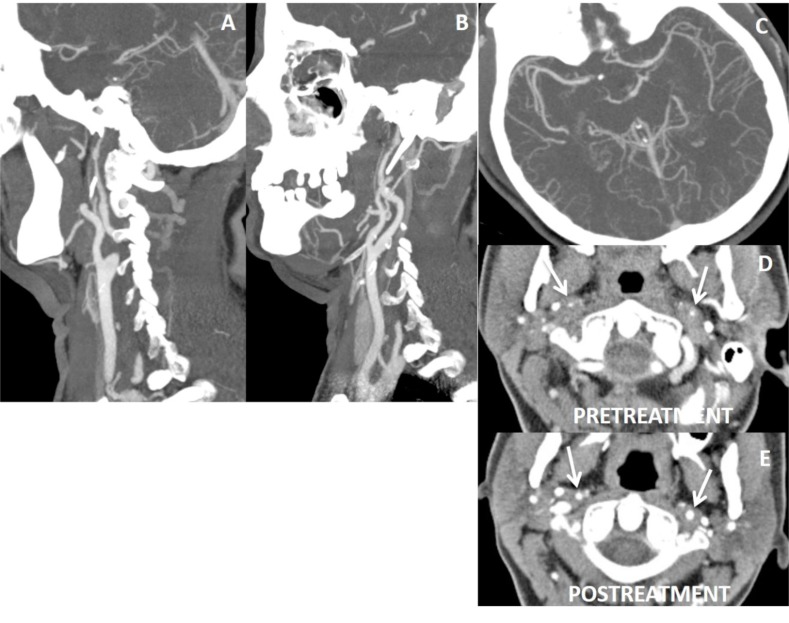
40 year’s old female with fibromuscular dysplasia, irregularities with luminal narrowing of both ICAs (A, B) and left M1 (C) are present on CTA. Axial CTA shows diffuse concentric thickening of wall of ICAs with luminal narrowing (arrows on D). Fat saturated T1W images did not reveal any hyperintensity suggesting intramural hematoma (not shown here). Following steroid treatment, wall thickening of ICAs lessens and their luminal diameter gets increased comparing to the pretreatment appearances (arrows on E). Note is that multiple vessels and long segment involvement are suggestive of vasculitis.
There is narrowing of left ICA on MRA (A) and CTA (B) with limitation of left MCA flow on CTA (C), but on CTA, bony contours (arrows on D) of ICAs at the skull base demonstrate left ICA being hypoplastic congenitally.
Ulcerated atherosclerotic plaque may give false appearance of pseudoaneurysm.
False tapering sign appearance of left ICA (A). There is thrombotic occlusion of left carotid terminus extending into M1 segment (B, C). After endovascular thrombolysis (D, E), left ICA return to normal. In fat suppressed T1 obtained before thrombolysis did not yield neither mural T1 hyperintensity nor increase in external diameter of left ICA comparing the right ICA (arrows on F) that would suggest dissection, but intramural hematoma will not be hyperintense in acute stage, external diameters of ICAs are more helpfull in this stage.
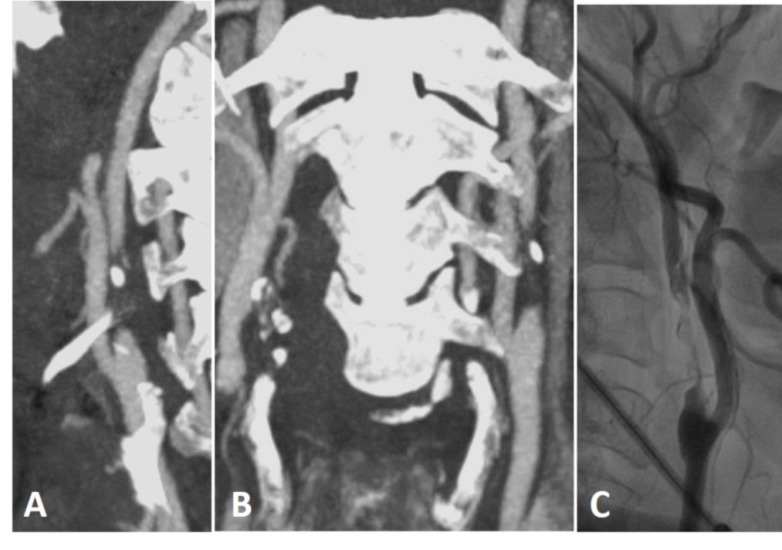
Thrombotic occlusion of left ICA on CTA (A, B) and DSA (C) are seen. Blunted ends of occlusion are against the dissection.
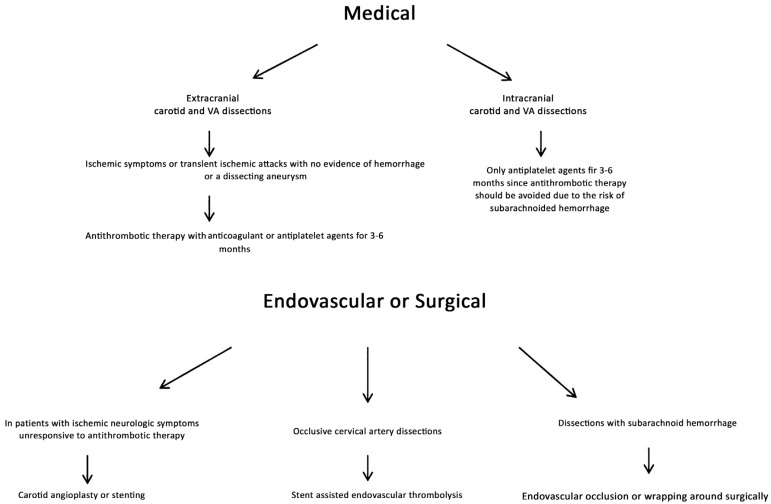
The flow chart shows treatment approaches in CCDs.
References
-
- Nagumo K. N akamori A, Kojima S. Rinsho Shinkeigaku. 2003;43:313–321. [Spontaneous intracranial internal carotid artery dissection: 6 case reports and a review of 39 cases in the literature]. - PubMed
-
- Volker W., Besselmann M., Dittrich R., et al. Generalized arteriopathy in patients with cervical artery dissection. Neurology. 2005;64:1508–1513. - PubMed
-
- Fusca M.R., Harrigan M.R. Cerebrovascular dissections--a review part I: Spontaneous dissections. Neurosurgery. 2011;68:242–257. - PubMed
-
- Benninger D.H., Gandjour J., Georgiadis D., et al. Benign long-term outcome of conservatively treated cervical aneurysms due to carotid dissection. Neurology. 2007;69:486–487. - PubMed
-
- Caso V., Paciaroni M., Corea F., et al. Recanalization of cervical artery dissection: influencing factors and role in neurological outcome. Cerebrovasc. Dis. 2004;17:93–97. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources