

Pituitary Apoplexy Presenting as Ophthalmoplegia and Altered Level of Consciousness without Headache
- PMID: 29854489
- PMCID: PMC5966706
- DOI: 10.1155/2018/7124364
Pituitary Apoplexy Presenting as Ophthalmoplegia and Altered Level of Consciousness without Headache
Abstract
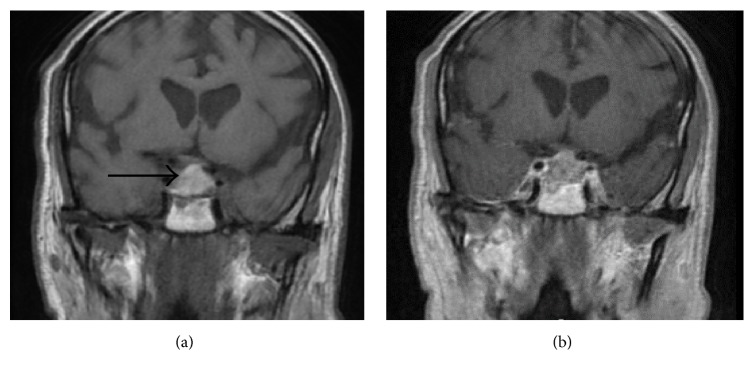
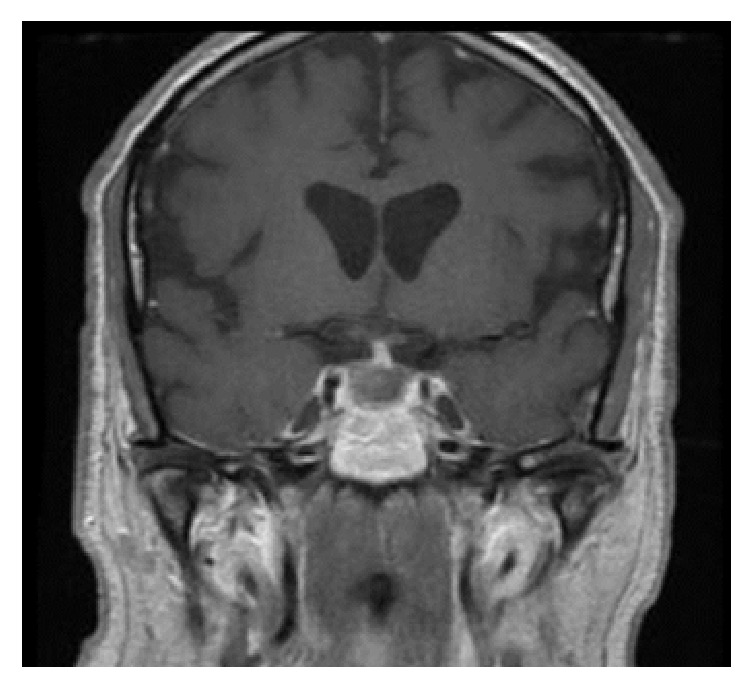
Background. Pituitary apoplexy (PA) is a clinical syndrome caused by acute ischemic infarction or hemorrhage of the pituitary gland. The typical clinical presentation of PA includes acute onset of severe headache, visual disturbance, cranial nerve palsy, and altered level of consciousness. Case Report. A 78-year-old man presented to the emergency department with one-day history of ptosis and diplopia and an acute-onset episode of altered level of consciousness which was resolving. He denied having headache, nausea, or vomiting. Physical examination revealed third-cranial nerve palsy and fourth-cranial nerve palsy both on the right side. Noncontrast computed tomography (CT) scan of the head was unremarkable. Brain magnetic resonance imaging (MRI) showed a pituitary mass with hemorrhage (apoplexy) and extension to the right cavernous sinus. The patient developed another episode of altered level of consciousness in the hospital. Transsphenoidal resection of the tumor was done which resulted in complete recovery of the ophthalmoplegia and mental status. Conclusion. Pituitary apoplexy can present with ophthalmoplegia and altered level of consciousness without having headache, nausea, or vomiting. A CT scan of the head could be negative for hemorrhage. A high index of suspicion is needed for early diagnosis and timely management of pituitary apoplexy.
Figures
References
-
- Bahmani Kashkouli M., Khalatbari M. R., Yahyavi S. T., Borghei-Razavi H., Soltan-Sanjari M. Pituitary apoplexy presenting as acute painful isolated unilateral third cranial nerve palsy. 2008;11(4):466–468. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
