

Statin Utilization Patterns and Outcomes for Patients with Acute Coronary Syndrome During and Following Inpatient Admissions
- PMID: 29855748
- PMCID: PMC6018577
- DOI: 10.1007/s10557-018-6800-3
Statin Utilization Patterns and Outcomes for Patients with Acute Coronary Syndrome During and Following Inpatient Admissions
Abstract
Purpose: High-intensity statins (HIS) are recommended by current treatment guidelines for patients with clinical atherosclerotic cardiovascular disease and should be administered soon after an acute coronary syndrome (ACS) event and maintained thereafter. However, adherence to guidelines remains adequate. Statin utilization patterns during index hospitalization and the first year after ACS event, and the association between statin utilization and post-discharge clinical and economic outcomes, are described.
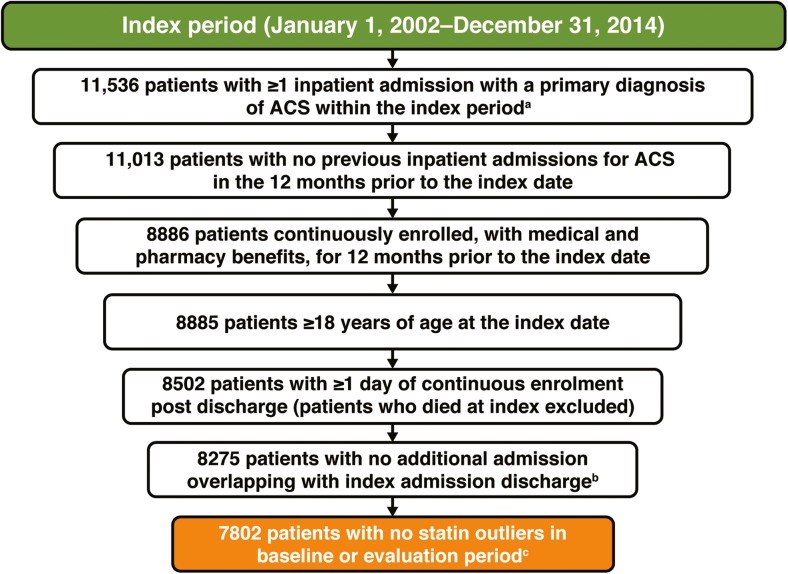
Methods: Retrospective, observational study of US adults from the MarketScan Research Databases (2002-2014) with ≥ 1 inpatient admission for ACS and no evidence of previous ACS event < 12 months prior to index.
Results: In total, 7802 patients met inclusion criteria. The most common index hospitalization primary diagnosis was myocardial infarction (94.6%). In the 3-month period before ACS admission, 3.4 and 14.9% of patients received HIS or low-to-moderate intensity statin, versus 13.2 and 30.7% during index hospitalization, and 16.4 and 45.1% in the year of follow-up. Of 1336 patients with a statin prescription filled on/after discharge, 53.2% filled prescriptions within 15 days of discharge and 14.9% delayed for > 91 days. The most common post-index hospital admissions for cardiovascular events were due to recurrent ACS (incidence rate = 115.2), heart failure (110.0), and revascularization (76.4). During follow-up, 2355 patients (30.2%) had all-cause inpatient admissions and 1136 (14.6%) had cardiovascular-specific admissions; mean all-cause medical and healthcare costs were $2456 and $2870, respectively, per patient per month.
Conclusions: Statin dosing and utilization of HIS remains lower than recommended in current treatment guidelines, leaving patients at considerable risk of subsequent cardiovascular events.
Keywords: Acute coronary syndrome; Cardiovascular events; Statin.
Conflict of interest statement
Conflict of Interest
Ms. Boklage is an employee of and stockholder in Regeneron Pharmaceuticals, Inc. Dr. Elassal was an employee of and stockholder in Regeneron Pharmaceuticals, Inc. at the time the study was conducted. Dr. Ding, Ms. Malangone-Monaco, Ms. Lopez-Gonzalez, and Ms. Henriques are employees of Truven Health Analytics, an IBM company, which was provided funding to conduct this study on behalf of Regeneron Pharmaceuticals, Inc. and Sanofi.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures


References
-
- Kolansky DM. Acute coronary syndromes: morbidity, mortality, and pharmacoeconomic burden. Am J Manag Care. 2009;15(2 Suppl):S36–S41. - PubMed
-
- Motivala AA, Tamhane U, Ramanath VS, Saab F, Montgomery DG, Fang J, Kline-Rogers E, May N, Ng G, Froehlich J, Gurm H, Eagle KA. A prior myocardial infarction: how does it affect management and outcomes in recurrent acute coronary syndromes? Clin Cardiol. 2008;31(12):590–596. doi: 10.1002/clc.20356. - DOI - PMC - PubMed
-
- Murphy SA, Cannon CP, Wiviott SD, McCabe CH, Braunwald E. Reduction in recurrent cardiovascular events with intensive lipid-lowering statin therapy compared with moderate lipid-lowering statin therapy after acute coronary syndromes from the PROVE IT-TIMI 22 (Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis In Myocardial Infarction 22) trial. J Am Coll Cardiol 2009;54(25):2358–2362. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
