

Safety, tolerability and pharmacokinetics/pharmacodynamics of the adrenomedullin antibody adrecizumab in a first-in-human study and during experimental human endotoxaemia in healthy subjects
- PMID: 29856470
- PMCID: PMC6089825
- DOI: 10.1111/bcp.13655
Safety, tolerability and pharmacokinetics/pharmacodynamics of the adrenomedullin antibody adrecizumab in a first-in-human study and during experimental human endotoxaemia in healthy subjects
Abstract
Aims: Adrenomedullin (ADM) is an important regulator of endothelial barrier function and vascular tone, and may represent a novel treatment target in sepsis. The non-neutralizing ADM antibody adrecizumab has shown promising results in preclinical sepsis models. In the present study, we investigated the safety, tolerability and pharmacokinetics (PK)/pharmacodynamics of adrecizumab in a first-in-man study and in a second study during experimental human endotoxaemia.
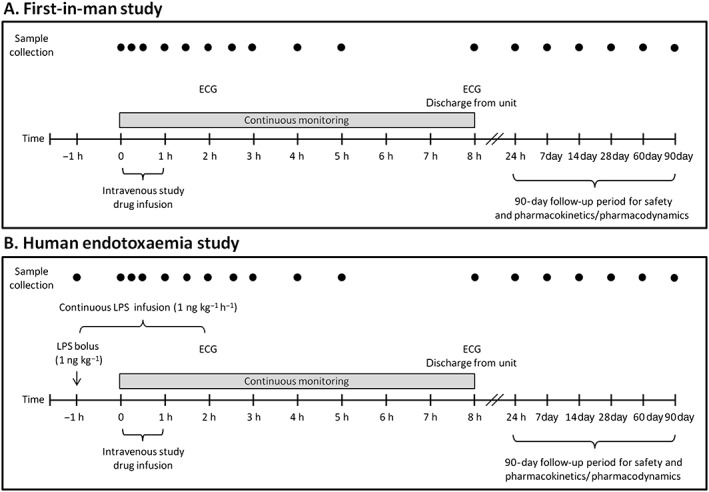
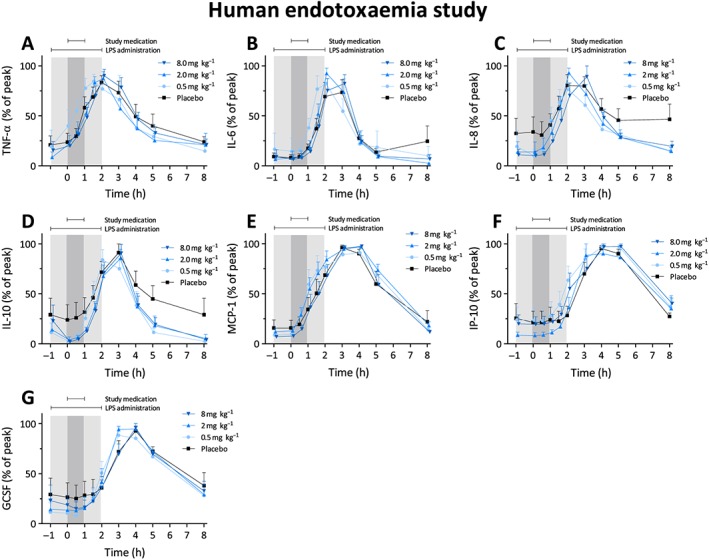
Methods: Forty-eight healthy male volunteers were enrolled in two randomized, double-blind, placebo-controlled phase I studies. In both studies, subjects received placebo or one of three doses of adrecizumab (n = 6 per group). In the second study, a bolus of 1 ng kg-1 endotoxin was followed by infusion of 1 ng kg-1 h-1 endotoxin for 3 h to induce systemic inflammation, and the study medication infusion started 1 h after endotoxin bolus administration.
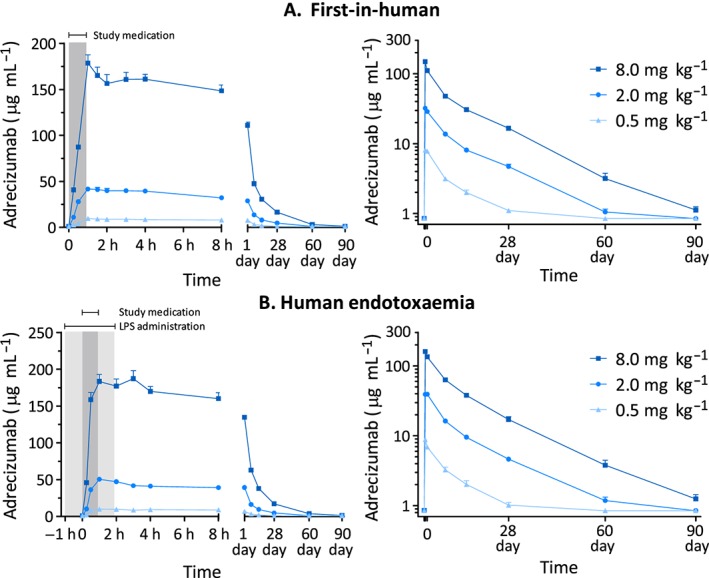
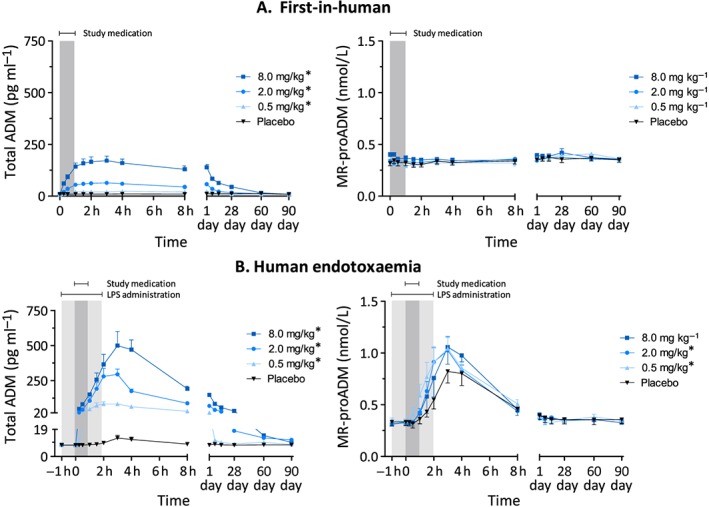
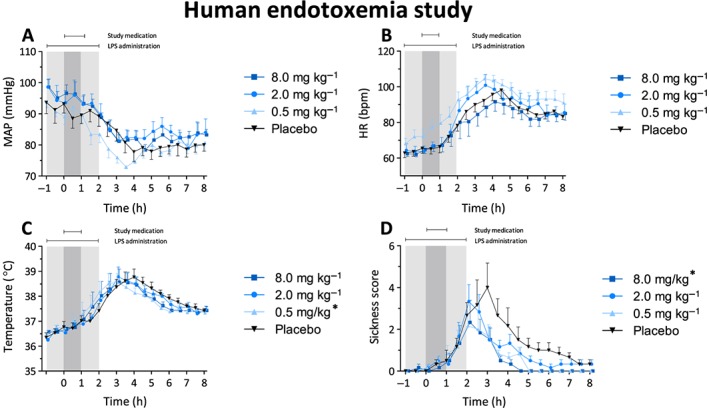
Results: Adrecizumab showed an excellent safety profile in both studies. PK analyses showed proportional increases in the maximum plasma concentration of adrecizumab with increasing doses, a small volume of distribution, a low clearance rate and a terminal half-life of ~14 days. adrecizumab elicited a pronounced increase in plasma ADM levels, whereas levels of mid-regional pro-adrenomedullin remained unchanged, indicating that de novo synthesis of ADM was not influenced. In the second study, no effects of adrecizumab on cytokine clearance were observed, whereas endotoxin-induced flu-like symptoms resolved more rapidly.
Conclusions: Administration of adrecizumab is safe and well tolerated in humans, both in the absence and presence of systemic inflammation. These findings pave the way for further investigation of adrecizumab in sepsis patients.
Keywords: adrecizumab; adrenomedullin; antibody; endotoxaemia; sepsis; shock.
© 2018 The British Pharmacological Society.
Figures
References
-
- Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, et al Assessment of global incidence and mortality of hospital‐treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med 2016; 193: 259–272. - PubMed
-
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med 2013; 41: 1167–1174. - PubMed
-
- Vincent JL, Marshall JC, Namendys‐Silva SA, Francois B, Martin‐Loeches I, Lipman J, et al Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med 2014; 2: 380–386. - PubMed
-
- Gotts JE, Matthay MA. Sepsis: pathophysiology and clinical management. BMJ 2016; 353: i1585. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
