

Exercise gas exchange in continuous-flow left ventricular assist device recipients
- PMID: 29856742
- PMCID: PMC5983474
- DOI: 10.1371/journal.pone.0187112
Exercise gas exchange in continuous-flow left ventricular assist device recipients
Abstract
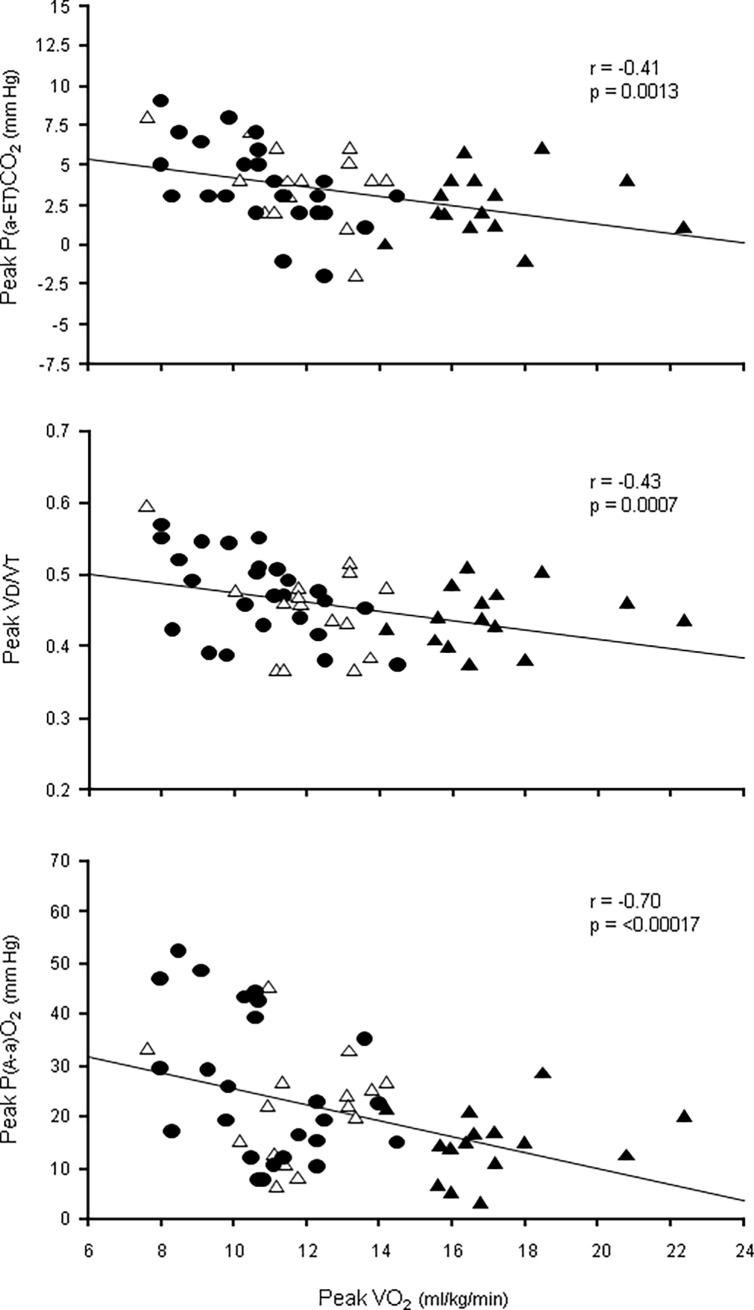
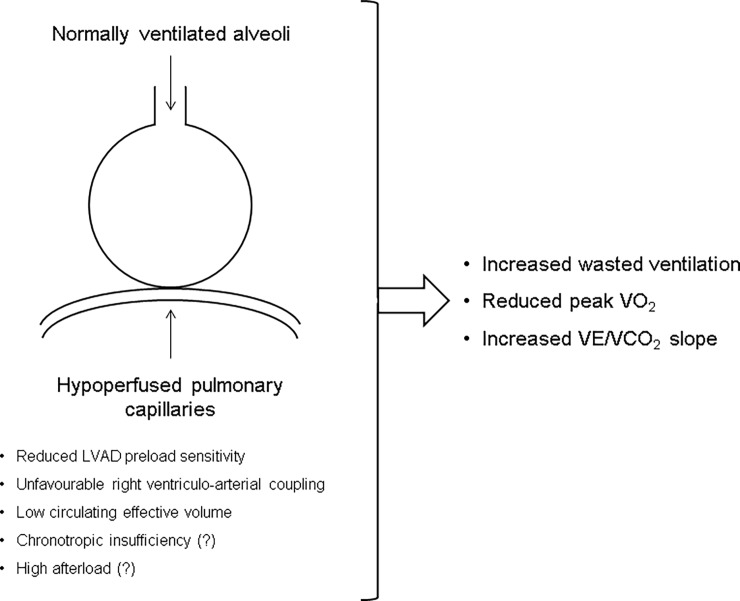
Exercise ventilation/perfusion matching in continuous-flow left ventricular assist device recipients (LVAD) has not been studied systematically. Twenty-five LVAD and two groups of 15 reduced ejection fraction chronic heart failure (HFrEF) patients with peak VO2 matched to that of LVAD (HFrEF-matched) and ≥14 ml/kg/min (HFrEF≥14), respectively, underwent cardiopulmonary exercise testing with arterial blood gas analysis, echocardiogram and venous blood sampling for renal function evaluation. Arterial-end-tidal PCO2 difference (P(a-ET)CO2) and physiological dead space-tidal volume ratio (VD/VT) were used as descriptors of alveolar and total wasted ventilation, respectively. Tricuspid annular plane systolic excursion/pulmonary artery systolic pressure ratio (TAPSE/PASP) and blood urea nitrogen/creatinine ratio were calculated in all patients and used as surrogates of right ventriculo-arterial coupling and circulating effective volume, respectively. LVAD and HFrEF-matched showed no rest-to-peak change of P(a-ET)CO2 (4.5±2.4 vs. 4.3±2.2 mm Hg and 4.1±1.4 vs. 3.8±2.5 mm Hg, respectively, both p >0.40), whereas a decrease was observed in HFrEF≥14 (6.5±3.6 vs. 2.8±2.0 mm Hg, p <0.0001). Rest-to-peak changes of P(a-ET)CO2 correlated to those of VD/VT (r = 0.70, p <0.0001). Multiple regression indicated TAPSE/PASP and blood urea nitrogen/creatinine ratio as independent predictors of peak P(a-ET)CO2. LVAD exercise gas exchange is characterized by alveolar wasted ventilation, i.e. hypoperfusion of ventilated alveoli, similar to that of advanced HFrEF patients and related to surrogates of right ventriculo-arterial coupling and circulating effective volume.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Daneshmand MA, Rajagopal K, Lima B, Khorram N, Blue LJ, Lodge AJ, et al. Left ventricular assist device destination therapy versus extended criteria cardiac transplant. Ann Thorac Surg. 2010;89(4):1205–1209; discussion 1210. doi: 10.1016/j.athoracsur.2009.12.058 - DOI - PubMed
-
- Holman WL, Naftel DC, Eckert CE, Kormos RL, Goldstein DJ, Kirklin JK. Durability of left ventricular assist devices: Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) 2006 to 2011. J. Thorac Cardiovasc Surg. 2013;146(2):437–441. doi: 10.1016/j.jtcvs.2013.02.018 - DOI - PubMed
-
- Westaby S. Rotary blood pumps as definitive treatment for severe heart failure. Future Cardiol. 2013;9(2):199–213. doi: 10.2217/fca.12.89 - DOI - PubMed
-
- Abshire M, Dennison Himmelfarb CR, Russell SD. Functional status in left ventricular assist device-supported patients: a literature review. J Card Fail. 2014;20(12):973–983. doi: 10.1016/j.cardfail.2014.08.011 - DOI - PMC - PubMed
-
- Compostella L, Russo N, Setzu T, Compostella C, Bellotto F. Exercise performance of chronic heart failure patients in the early period of support by an axial-flow left ventricular assist device as destination therapy. Artif Organs. 2014;38(5):366–373. doi: 10.1111/aor.12172 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
