

Low-molecular-weight heparin venous thromboprophylaxis in critically ill patients with renal dysfunction: A subgroup analysis of the PROTECT trial
- PMID: 29856817
- PMCID: PMC5983525
- DOI: 10.1371/journal.pone.0198285
Low-molecular-weight heparin venous thromboprophylaxis in critically ill patients with renal dysfunction: A subgroup analysis of the PROTECT trial
Abstract
Introduction: There is concern about excessive bleeding when low-molecular-weight heparins (LMWHs) are used for venous thromboembolism (VTE) prophylaxis in renal dysfunction. Our objective was to evaluate whether LMWH VTE prophylaxis was safe and effective in critically ill patients with renal dysfunction by conducting a subgroup analysis of PROTECT, a randomized blinded trial.
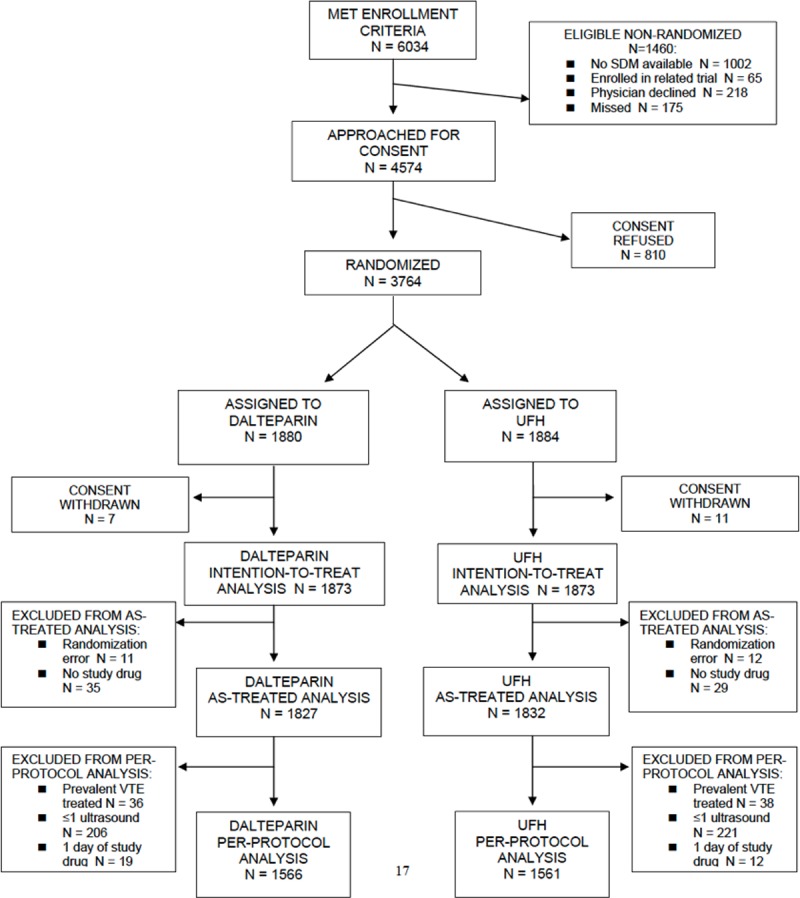
Methods: We studied intensive care unit (ICU) patients with pre-ICU dialysis-dependent end-stage renal disease (ESRD; pre-specified subgroup; n = 118), or severe renal dysfunction at ICU admission (defined as ESRD or non-dialysis dependent with creatinine clearance [CrCl] <30 ml/min; post hoc subgroup; n = 590). We compared dalteparin, 5000 IU daily, with unfractionated heparin (UFH), 5000 IU twice daily, and considered outcomes of proximal leg deep vein thrombosis (DVT); pulmonary embolism (PE); any VTE; and major bleeding. Adjusted hazard ratios [HR] were calculated using Cox regression.
Results: In patients with ESRD, there was no significant difference in DVT (8.3% vs. 5.2%, p = 0.76), any VTE (10.0% vs. 6.9%; p = 0.39) or major bleeding (5.0% vs. 8.6%; p = 0.32) between UFH and dalteparin. In patients with severe renal dysfunction, there was no significant difference in any VTE (10.0% vs. 6.4%; p = 0.07) or major bleeding (8.9% vs. 11.0%; p = 0.66) but an increase in DVT with dalteparin (7.6% vs. 3.7%; p = 0.04). Interaction p-values for comparisons of HRs (ESRD versus not) were non-significant.
Conclusions: In critically ill patients with ESRD, or severe renal dysfunction, there was no significant difference in any VTE or major bleeding between UFH and dalteparin. Patients with severe renal dysfunction who received dalteparin had more proximal DVTs than those on UFH; this finding did not hold in patients with ESRD alone.
Conflict of interest statement
This study received support from Pfizer Canada, which provided dalteparin for Canadian centers, and Eisai, Inc, which provided dalteparin for centers in the United States. Neither group played a role in the design, conduct, analysis, interpretation or write-up of this trial. The authors have no other relevant declarations relating to employment, consultancy, patents, products in development, or marketed products. The competing interests declared here do not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Kaplan D, Casper TC, Elliott CG, Men S, Pendleton RC, Kraiss LW, et al. VTE Incidence and Risk Factors in Patients With Severe Sepsis and Septic Shock. Chest. 2015;148(5):1224–30. doi: D—NLM: PMC4631038 [Available on 11/01/16] EDAT- 2015/06/26 06:00 MHDA- 2016/02/19 06:00 CRDT- 2015/06/26 06:00 AID - S0012-3692(15)50233-X [pii] AID—doi: 10.1378/chest.15-0287 [doi] PST—ppublish. - DOI - PMC - PubMed
-
- Protect Investigators for the Canadian Critical Care Trials Group, The Australian New Zealand Intensive Care Society Clinical Trials Group, Cook D, Meade M, Guyatt G, Walter S, et al. Dalteparin versus unfractionated heparin in critically ill patients. The New England journal of medicine. 2011;364(14):1305–14. Epub 2011/03/23. doi: 10.1056/NEJMoa1014475 . - DOI - PubMed
-
- Kahn SR, Lim W, Dunn AS, Cushman M, Dentali F, Akl E, et al. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e195S–226S. doi: D—NLM: PMC3278052 EDAT- 2012/02/15 06:00 MHDA- 2012/04/14 06:00 CRDT- 2012/02/09 06:00 AID - S0012-3692(12)60124-X [pii] AID—doi: 10.1378/chest.11-2296 [doi] PST—ppublish. - DOI - PMC - PubMed
-
- Linkins LA, Dans AL, Moores LK, Bona R, Davidson BL, Schulman S, et al. Treatment and prevention of heparin-induced thrombocytopenia: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e495S–530S. Epub 2012/02/15. doi: 10.1378/chest.11-2303 ; PubMed Central PMCID: PMCPMC3278058. - DOI - PMC - PubMed
-
- Boneu B, Caranobe C, Sie P. Pharmacokinetics of heparin and low molecular weight heparin. Bailliere's Clin Haematol. 1990;3:531–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
